Sleep is a reversible, naturally recurring state of reduced consciousness and voluntary muscle inactivity, regulated by two independent biological systems - the circadian rhythm (a roughly 24-hour internal clock) and sleep homeostasis (a pressure to sleep that builds the longer you stay awake).
Far from being passive rest, sleep is one of the most active and essential biological processes in the human body: during sleep, the brain consolidates memories, clears metabolic waste through the glymphatic system, regulates hormones, processes emotional experiences, and rebuilds neural connections.
The average human spends approximately one-third of their life asleep, and research over the past seven decades has demonstrated that this time is not optional overhead but a fundamental requirement for cognitive performance, immune function, metabolic health, and longevity.
For most of human history, sleep was poorly understood. Aristotle thought sleep was caused by vapors rising from the stomach after eating. Descartes believed the brain literally deflated during sleep.
As recently as the mid-20th century, sleep research was not considered a serious scientific discipline - the prevailing view was that sleep was simply a passive state of unconsciousness during which nothing interesting happened.
Then, in 1953, a graduate student named Eugene Aserinsky noticed something remarkable while monitoring the eyes of sleeping subjects in the laboratory of Nathaniel Kleitman at the University of Chicago. During certain phases of sleep, the eyes moved rapidly beneath closed lids - not randomly but in coordinated bursts.
Kleitman recognized the significance immediately: the brain was not simply "off" during sleep. Something active was happening.
Their discovery of REM (Rapid Eye Movement) sleep, published in Science in 1953, launched modern sleep science and opened the door to understanding sleep as one of the most complex and important processes in biology.
What researchers have found in the seven decades since is extraordinary. Sleep is an orchestrated sequence of distinct physiological stages, each serving different functions, regulated by molecular clocks in every cell of the body, and so essential to survival that every animal with a nervous system does it - even fruit flies, jellyfish, and roundworms.
"The shorter your sleep, the shorter your life. The leading causes of disease and death in developed nations - diseases that are crippling health care systems - all have recognized causal links to a lack of sleep."
- Matthew Walker, Why We Sleep: Unlocking the Power of Sleep and Dreams (2017)
The Two-Process Model: How Your Body Decides When to Sleep
Modern sleep science understands sleep timing and depth through the two-process model, proposed by Swiss sleep researcher Alexander Borbely in 1982 and published in Human Neurobiology.
The model describes the interaction of two independent biological systems that together determine when you feel sleepy, when you wake up, and how deeply you sleep.
Process C: The Circadian Drive
The circadian rhythm is an approximately 24-hour biological cycle governing sleep-wake timing, body temperature, hormone release, and dozens of other physiological processes. The word comes from Latin: circa (around) + dies (day).
Nearly every cell in the body contains molecular clock machinery - genes called clock genes (including CLOCK, BMAL1, PER, and CRY) that create self-sustaining oscillations of protein production and degradation on a roughly 24-hour cycle.
These cellular clocks are coordinated by a master pacemaker: the suprachiasmatic nucleus (SCN), a tiny paired structure in the hypothalamus containing approximately 20,000 neurons.
The SCN receives light information directly from the retina through a dedicated neural pathway called the retinohypothalamic tract, using specialized light-sensitive cells called intrinsically photosensitive retinal ganglion cells (ipRGCs) that are distinct from the rods and cones used for vision.
These cells are particularly sensitive to short-wavelength (blue) light in the 460-480 nanometer range.
The SCN uses light information to synchronize the body's internal clock to the external light-dark cycle. In response to darkness, the SCN signals the pineal gland to secrete melatonin - a hormone that does not directly cause sleep but signals to the body that it is nighttime and adjusts the timing of sleep readiness.
Melatonin levels typically begin rising approximately 2 hours before habitual bedtime (a period called the dim light melatonin onset, or DLMO) and remain elevated throughout the night, dropping as morning light arrives.
The circadian system creates several notable features of daily experience:
- A "forbidden zone" for sleep in the late afternoon and early evening (approximately 5-8 PM for most adults), when circadian arousal peaks - paradoxically, this is when it is hardest to fall asleep, despite having been awake for many hours
- A "sleep gate" in the late evening when body temperature drops and melatonin rises, creating a window of strong sleep tendency
- A "second wind" if you stay up past the sleep gate - you feel temporarily more alert around 10-11 PM before sleepiness intensifies again
- The 2-3 PM post-lunch dip, which has nothing to do with lunch - it is a circadian feature present even in fasted individuals, a minor trough in the circadian alerting signal
Chronotype: Larks, Owls, and Genetic Variation
There is genuine genetic variation in circadian phase. "Larks" (morning chronotypes) have earlier phase positions - they naturally feel sleepy earlier in the evening and wake earlier in the morning. "Owls" (evening chronotypes) have later phases.
Research by geneticist Ying-Hui Fu at UCSF identified specific mutations in the PER2 and DEC2 genes associated with extreme early-morning chronotype (familial advanced sleep phase syndrome).
A 2019 genome-wide association study by Samuel Jones and colleagues, published in Nature Communications, identified 351 genetic loci associated with chronotype, confirming that sleep timing preferences are substantially heritable.
Teenagers deserve particular mention: adolescent circadian clocks are biologically delayed relative to adults.
Research by Mary Carskadon at Brown University, beginning in the 1990s and continuing through the 2020s, has demonstrated that the teenage circadian shift is not behavioral laziness but a genuine biological phenomenon - melatonin onset is later, the sleep gate opens later, and the circadian arousal peak extends later into the evening.
The American Academy of Pediatrics recommended in 2014 that middle and high schools start no earlier than 8:30 AM, citing this research.
California became the first U.S. state to mandate later school start times (8:30 AM for high schools) beginning in 2022.
Process S: Sleep Homeostasis
Parallel to the circadian process, sleep homeostasis tracks the accumulation of sleep pressure. The primary molecular signal is adenosine, a byproduct of cellular energy metabolism (specifically, the breakdown of adenosine triphosphate, or ATP) that accumulates in the brain during wakefulness.
The longer you have been awake, the higher your adenosine levels, and the more intensely you feel the drive to sleep.
When you sleep, adenosine is cleared - particularly rapidly during slow-wave sleep. This is why you feel refreshed after adequate sleep and groggy after sleep deprivation: you are working down accumulated adenosine in the first case and operating under a heavy adenosine load in the second.
Caffeine works by blocking adenosine receptors (specifically the A1 and A2A receptor subtypes), preventing adenosine from binding and signaling drowsiness. But caffeine does not clear adenosine - it merely masks it.
When caffeine is metabolized (half-life of approximately 5-7 hours in most adults, though this varies significantly by genotype - variants in the CYP1A2 gene can produce half-lives ranging from 2 to 12 hours), the accumulated adenosine floods back onto receptors, producing the familiar caffeine "crash." Regular caffeine consumption leads to upregulation of adenosine receptors, requiring more caffeine to achieve the same blocking effect - tolerance - and making withdrawal (when all that accumulated adenosine suddenly has unblocked access to upregulated receptors) particularly unpleasant.
Sleep Architecture: What Happens Each Night
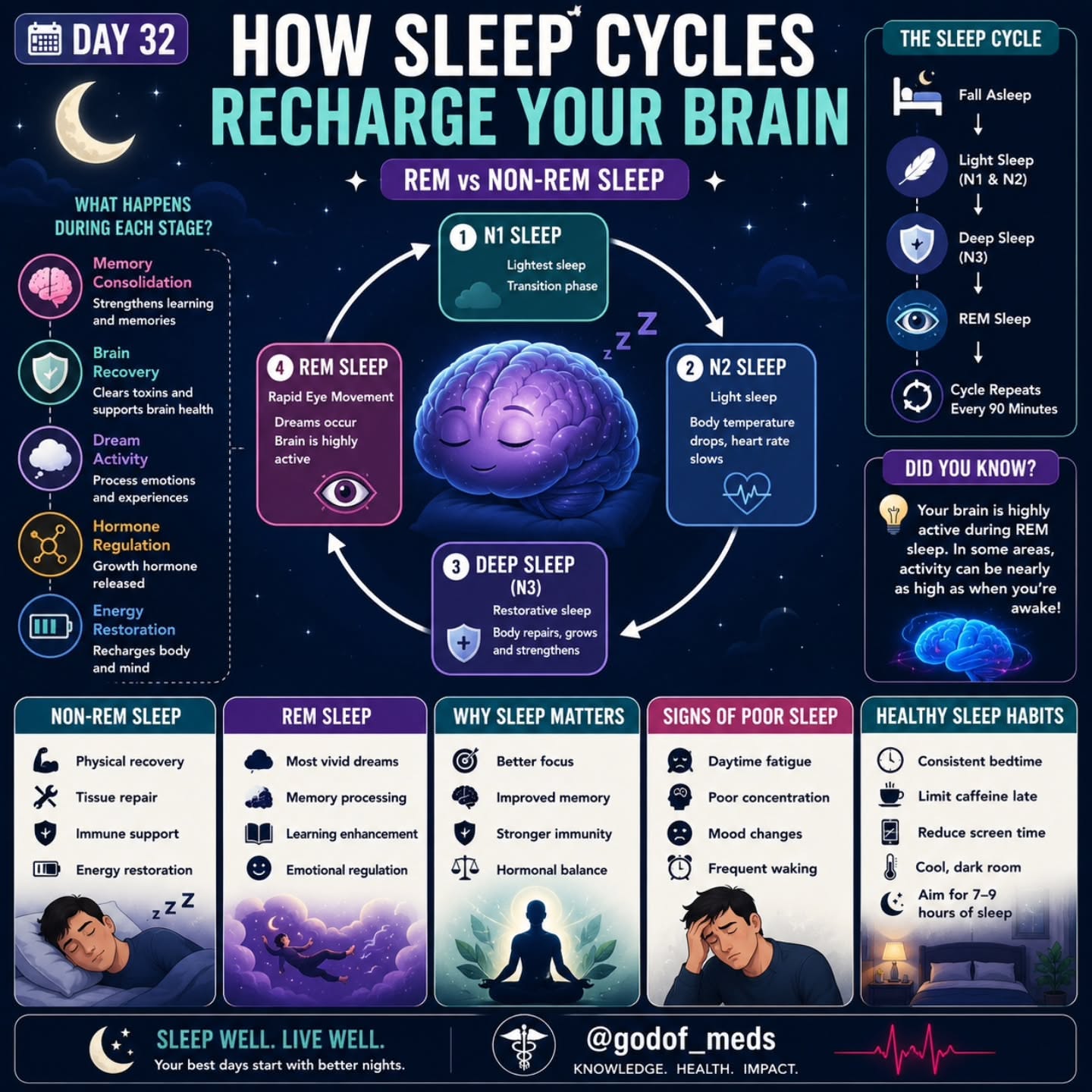
A normal adult sleep episode consists of 4-6 cycles, each approximately 90 minutes long, cycling through NREM (Non-Rapid Eye Movement) stages and REM (Rapid Eye Movement) sleep in a predictable pattern.
The composition of these cycles changes across the night in a critically important way: early cycles are dominated by deep NREM sleep (N3), while later cycles are dominated by REM sleep.
| Sleep Stage | Duration per Cycle | % of Total Sleep | Brain Activity | Key Functions |
|---|---|---|---|---|
| N1 (Light sleep) | 1-7 minutes | ~5% | Theta waves (4-7 Hz) | Transition from wakefulness |
| N2 (Intermediate) | 10-25 minutes | ~50% | Sleep spindles, K-complexes | Memory consolidation, sleep maintenance |
| N3 (Slow-wave deep) | 20-40 minutes (early cycles) | ~20% | Delta waves (0.5-4 Hz) | Physical restoration, immune function, waste clearance |
| REM | 10-60 minutes (increases) | ~25% | Beta/gamma (near-waking) | Emotional processing, procedural learning, dreaming |
N1: The Threshold
N1 is the lightest stage of sleep - the transition from wakefulness. Brain activity shifts from waking alpha waves (8-12 Hz) and beta waves (12-30 Hz) to slower theta waves (4-7 Hz). Muscle tone decreases gradually.
Hypnic jerks - the sudden involuntary muscle contractions sometimes experienced when falling asleep - occur in N1 and are thought to result from the brain misinterpreting the sudden muscle relaxation as falling.
N1 typically lasts 1-7 minutes per cycle and you can be easily awakened from it; many people woken from N1 report that they were not actually asleep.
N2: The Workhorse of Sleep
N2 is true sleep but not the deepest. It comprises approximately 50% of total sleep time - more than any other stage. The EEG (electroencephalogram) shows two characteristic features:
Sleep spindles - bursts of oscillatory neural activity at 12-15 Hz, lasting 0.5-3 seconds - are generated by the thalamo-cortical loop and appear to play a critical role in memory consolidation.
Research by Sara Mednick at UC Irvine (2013) and Bernhard Staresina at the University of Birmingham (2015) has demonstrated that sleep spindles facilitate the transfer of memories from the hippocampus (where they are initially encoded) to cortical long-term storage.
People with more spindles during post-learning sleep perform better on memory tests; conversely, reduced spindle activity is associated with age-related memory decline and is observed early in Alzheimer's disease.
K-complexes - large negative deflections followed by positive deflection - are thought to protect sleep from external stimuli by briefly suppressing cortical responsiveness. They also appear to play a role in memory consolidation and synaptic homeostasis.
N3: The Deep Restoration
N3 (also called slow-wave sleep or SWS) is the deepest stage of sleep. The EEG is dominated by large, slow delta waves (0.5-4 Hz) generated by the synchronized firing of large populations of cortical neurons.
Arousal threshold is highest - you are hardest to wake during N3, and being woken from it produces the most intense grogginess (called sleep inertia).
N3 is the most physically restorative stage:
- Growth hormone is secreted in pulses primarily during N3 by the anterior pituitary gland, driving tissue repair, protein synthesis, muscle growth, and metabolic regulation. Research by Eve Van Cauter at the University of Chicago (2000) demonstrated that sleep deprivation dramatically suppresses growth hormone secretion.
- Immune function: Natural killer cell activity, cytokine production, and immune memory consolidation are heightened during N3. A landmark 2009 study by Sheldon Cohen at Carnegie Mellon found that people sleeping fewer than 7 hours per night were 2.94 times more likely to develop a cold after experimental rhinovirus exposure than those sleeping 8+ hours.
- Glymphatic clearance: The glymphatic system - discovered by Maiken Nedergaard and colleagues at the University of Rochester in 2012 and published in Science Translational Medicine - is a waste clearance network that uses cerebrospinal fluid flowing through channels surrounding blood vessels to flush metabolic byproducts from the brain. During slow-wave sleep, the brain's interstitial space expands by approximately 60% and allowing dramatically more efficient clearance of waste products including amyloid-beta and tau - the proteins that accumulate in Alzheimer's disease. Nedergaard's 2013 paper in Science demonstrated that glymphatic clearance is approximately 10 times more active during sleep than during wakefulness.
- Metabolic regulation: Glucose metabolism and insulin sensitivity are partly regulated during sleep. Van Cauter's research showed that restricting sleep to 4 hours per night for just 6 nights produced glucose tolerance levels comparable to pre-diabetic states in healthy young adults.
N3 is most abundant in the first third of the night. Missing the first few hours of sleep means missing disproportionate N3 sleep - which is why going to bed late is biologically different from waking up early, even if total sleep hours are the same.
REM Sleep: The Paradoxical Stage
REM sleep is the stage most associated with vivid, narrative, emotionally intense dreaming. It was named for the rapid eye movements observed by Aserinsky and Kleitman in their 1953 discovery.
The brain during REM is remarkably active - EEG patterns show beta and gamma wave activity similar to wakefulness - yet the body is effectively paralyzed.
This REM atonia (muscle paralysis) is generated by signals from the brainstem (specifically the sublaterodorsal nucleus) that inhibit spinal motor neurons, preventing voluntary muscle movement.
Exceptions are made for the diaphragm (you must continue breathing), the extraocular muscles (producing the characteristic eye movements), and the middle ear muscles.
REM atonia evolved to prevent organisms from physically acting out their dreams. When this mechanism fails - a condition called REM sleep behavior disorder - people thrash, kick, and sometimes injure themselves or bed partners during vivid dreams.
REM periods get progressively longer through the night. The first REM period lasts only 5-10 minutes; the final REM period before natural waking may last 45-60 minutes. This means that cutting sleep short by even one hour disproportionately removes REM sleep - and with it, the functions that REM serves:
- Emotional memory processing: Research by Matthew Walker at UC Berkeley has proposed that REM sleep, characterized by the complete suppression of norepinephrine (the stress neurochemical), allows emotional memories to be reactivated and reprocessed in a neurochemically safe environment, gradually reducing their emotional charge while preserving the informational content. This theory explains why "sleeping on it" often makes emotional events feel less raw.
- Procedural and creative learning: REM sleep improves performance on tasks requiring pattern recognition and creative problem-solving. A 2004 study by Ullrich Wagner and colleagues at the University of Lubeck, published in Nature, found that subjects were 2.6 times more likely to discover a hidden pattern in a mathematical task after a night of sleep that included REM than after equivalent waking time.
- Neural development: REM sleep is proportionally far greater in neonates (approximately 50% of total sleep) and decreases with age. The relationship suggests a critical role in neural circuit development and synaptic pruning during early life.
For more on how dreams function, see why do we dream.
The Consequences of Sleep Deprivation
Acute Cognitive Impairment
The most well-characterized acute effect of sleep deprivation is cognitive impairment.
A landmark 1997 study by Drew Dawson and Kathryn Reid at the University of South Australia, published in Nature, found that after 17-19 hours of continuous wakefulness, performance on tests of attention, reaction time, and working memory degraded to levels equivalent to a blood alcohol concentration of 0.05% - legal impairment in most countries.
After 24 hours without sleep, performance was equivalent to a BAC of approximately 0.10% - above the legal driving limit in every U.S. state.
The most insidious finding in sleep deprivation research comes from Hans Van Dongen and David Dinges at the University of Pennsylvania.
Their 2003 study, published in Sleep, found that people sleeping 6 hours per night for two weeks showed cumulative cognitive performance degradation equivalent to 24-48 hours of total sleep deprivation - but reported feeling only "slightly sleepy." They had lost the ability to accurately gauge how impaired they were.
This subjective adaptation without objective recovery is one of the most dangerous features of chronic sleep restriction: people genuinely believe they have adapted to short sleep when performance data shows they have not.
Long-Term Health Consequences
Chronic sleep deprivation is not merely inconvenient - it is a documented risk factor for the leading causes of death and disability in developed nations:
| Condition | Effect of Chronic Short Sleep | Key Evidence |
|---|---|---|
| Cardiovascular disease | 45% increased heart attack risk (< 6 hours/night) | Cappuccio et al., 2011, European Heart Journal |
| Obesity | Disrupts leptin/ghrelin balance; increases hunger and caloric intake | Spiegel et al., 2004, Annals of Internal Medicine |
| Type 2 diabetes | Impairs insulin sensitivity; alters glucose metabolism | Van Cauter et al., 2008, The Lancet |
| Alzheimer's disease | Impairs glymphatic clearance of amyloid-beta | Xie et al., 2013, Science; Shokri-Kojori et al., 2018, PNAS |
| Cancer | Short sleep associated with increased colorectal, breast, prostate cancer risk | WHO classification of night shift work as "probably carcinogenic" (2007) |
| Depression and anxiety | Strong bidirectional relationship; sleep disruption both causes and results from mood disorders | Baglioni et al., 2011, Journal of Affective Disorders |
| Immune function | Single night of 4-hour sleep reduces natural killer cell activity by 70% | Irwin et al., 1996, FASEB Journal |
A comprehensive 2010 meta-analysis by Francesco Cappuccio and colleagues at the University of Warwick, published in Sleep, analyzed 16 prospective studies covering 1.3 million participants and found that sleeping fewer than 6 hours per night was associated with a 12% increased risk of all-cause mortality.
The optimal sleep duration for lowest mortality risk was consistently 7-8 hours. Sleeping more than 9 hours was also associated with increased mortality, though this likely reflects underlying illness rather than a causal effect of long sleep.
The relationship between sleep deprivation and cognitive decline is particularly concerning given the aging population.
Research published in PNAS (Shokri-Kojori et al., 2018) used PET imaging to demonstrate that a single night of sleep deprivation produced measurable increases in amyloid-beta accumulation in the human brain - a finding with profound implications for the relationship between chronic sleep disruption and Alzheimer's risk.
How to Sleep Better: Evidence-Based Recommendations
Sleep hygiene - the practices and environmental conditions that promote consistent, restorative sleep - has a strong evidence base. The following recommendations are supported by controlled studies and clinical evidence:
Light Management
Morning bright light (ideally sunlight, at least 10,000 lux for 20-30 minutes) advances the circadian phase and improves sleep timing. Research by Charles Czeisler at Harvard Medical School has demonstrated that light is the single most powerful signal for circadian entrainment.
Evening light restriction is equally important. Blue-wavelength light (from screens, LED lighting, and fluorescent bulbs) suppresses melatonin production.
A 2014 study by Anne-Marie Chang and colleagues at Brigham and Women's Hospital, published in PNAS, found that reading on an iPad before bed delayed melatonin onset by approximately 1.5 hours, delayed circadian phase, reduced REM sleep, and impaired next-morning alertness compared to reading a printed book.
Practical steps: maximize daylight exposure in the first 1-2 hours after waking; begin dimming lights and switching to warm-toned light 1-2 hours before intended sleep; consider blue-light filtering (f.lux, Night Shift, or hardware-level filtering) for evening screen use, though reducing screen time entirely is more effective.
Temperature
Core body temperature must fall approximately 1-2 degrees Celsius to initiate and maintain sleep. A cool bedroom (65-68 degrees F / 18-20 degrees C) facilitates this thermal decline.
Research by Eus van Someren at the Netherlands Institute for Neuroscience has shown that skin warming (which paradoxically accelerates core cooling by drawing blood to the body surface) improves sleep onset.
This explains why warm baths or showers approximately 60-90 minutes before bed improve sleep - they accelerate the core temperature drop that signals the body to initiate sleep.
Consistency
A regular sleep-wake schedule - including weekends - maintains circadian alignment and reduces social jet lag (the misalignment between social schedules and biological clocks that affects an estimated 87% of the adult population to some degree, according to research by Till Roenneberg at Ludwig Maximilian University of Munich).
Going to bed at 11 PM on weekdays and 2 AM on weekends creates the equivalent of weekly transatlantic travel for the circadian system.
Caffeine Timing
Given caffeine's half-life of 5-7 hours (and longer in some genotypes), coffee consumed at 2 PM still has 25-50% of its caffeine in your system at 10 PM. Cutting caffeine after noon or early afternoon significantly improves sleep for most people.
A 2013 study by Christopher Drake at Wayne State University, published in the Journal of Clinical Sleep Medicine, found that caffeine consumed even 6 hours before bedtime significantly reduced total sleep time and sleep efficiency.
Alcohol
Alcohol is the most commonly used sleep aid among adults, but it substantially disrupts sleep architecture.
Research by Irshaad Ebrahim and colleagues (2013), published in Alcoholism: Clinical and Experimental Research, reviewed 27 studies and found that alcohol at any dose suppresses REM sleep, fragments sleep in the second half of the night (producing frequent awakenings), and disrupts the normal cycling between sleep stages.
What people experience as "good sleep" after drinking is deep early NREM - but at the cost of REM, sleep continuity, and restorative sleep quality.
For practical guidance on improving your sleep habits, see how to fix your sleep. For data on sleep patterns across the population, see sleep statistics 2026. For understanding how sleep relates to memory consolidation and brain aging, those articles explore the connections in depth.
Sources & Further Reading
- Walker, Matthew P. (2017). Why We Sleep: Unlocking the Power of Sleep and Dreams. Scribner. ISBN 978-1501144325
- Borbely, Alexander A. (1982). "A Two Process Model of Sleep Regulation." Human Neurobiology, 1(3), 195-204.
- Aserinsky, Eugene and Nathaniel Kleitman. (1953). "Regularly Occurring Periods of Eye Motility, and Concomitant Phenomena, During Sleep." Science, 118(3062), 273-274. doi.org/10.1126/science.118.3062.273
- Xie, Lulu, et al. (2013). "Sleep Drives Metabolite Clearance from the Adult Brain." Science, 342(6156), 373-377. doi.org/10.1126/science.1241224
- Cappuccio, Francesco P., et al. (2010). "Sleep Duration and All-Cause Mortality: A Systematic Review and Meta-Analysis of Prospective Studies." Sleep, 33(5), 585-592. doi.org/10.1093/sleep/33.5.585
- Van Dongen, Hans P.A., et al. (2003). "The Cumulative Cost of Additional Wakefulness: Dose-Response Effects on Neurobehavioral Functions and Sleep Physiology." Sleep, 26(2), 117-126.
- Dawson, Drew and Kathryn Reid. (1997). "Fatigue, Alcohol and Performance Impairment." Nature, 388, 235. doi.org/10.1038/40775
- Wagner, Ullrich, et al. (2004). "Sleep Inspires Insight." Nature, 427, 352-355. doi.org/10.1038/nature02223
- Chang, Anne-Marie, et al. (2014). "Evening Use of Light-Emitting eReaders Negatively Affects Sleep, Circadian Timing, and Next-Morning Alertness." Proceedings of the National Academy of Sciences, 112(4), 1232-1237.
- Jones, Samuel E., et al. (2019). "Genome-Wide Association Analyses of Chronotype in 697,828 Individuals Provides Insights into Circadian Rhythms." Nature Communications, 10, 343.
- Cohen, Sheldon, et al. (2009). "Sleep Habits and Susceptibility to the Common Cold." Archives of Internal Medicine, 169(1), 62-67.
- Drake, Christopher, et al. (2013). "Caffeine Effects on Sleep Taken 0, 3, or 6 Hours Before Going to Bed." Journal of Clinical Sleep Medicine, 9(11), 1195-1200.
- Nedergaard, Maiken. (2013). "Neuroscience: Garbage Truck of the Brain." Science, 340(6140), 1529-1530.
- Stickgold, Robert and Matthew P. Walker. (2013). "Sleep-Dependent Memory Triage." Nature Neuroscience, 16(2), 139-145.
- Carskadon, Mary A. (2011). "Sleep in Adolescents: The Perfect Storm." Pediatric Clinics of North America, 58(3), 637-647.
Health note: This article is general educational information about how a topic works, not medical, psychological, or mental-health advice, diagnosis, or treatment. Everyone's situation is different, and research findings describe groups, not individuals.
If you are struggling or have concerns about your health, please talk to a qualified professional such as a doctor or licensed therapist.
If you are in crisis or thinking about harming yourself, contact your local emergency services or a crisis line right away, in the US you can call or text 988 (Suicide & Crisis Lifeline); elsewhere, find local lines at findahelpline.com.
Frequently Asked Questions
Why do we need sleep at all?
Sleep serves multiple essential functions: memory consolidation (transferring information from short to long-term memory), metabolic waste clearance from the brain via the glymphatic system, immune system strengthening, emotional regulation, tissue repair, and hormonal regulation. No single function explains all of sleep’s necessity, it appears to serve multiple critical roles simultaneously.
What are the different stages of sleep?
Sleep has two major types: NREM (Non-REM) sleep and REM sleep. NREM has three stages: N1 (light sleep, transition from wakefulness), N2 (deeper sleep with sleep spindles and K-complexes), and N3 (slow-wave deep sleep, most physically restorative). REM sleep has rapid eye movements, near-waking brain activity, muscle paralysis, and vivid dreaming. A normal night cycles through these stages 4-6 times.
How does the circadian rhythm control sleep?
The suprachiasmatic nucleus (SCN) in the hypothalamus is the brain’s master clock, synchronized primarily by light. In darkness, the pineal gland releases melatonin, signaling sleep time. Core body temperature drops. Cortisol peaks near dawn. This 24-hour cycle interacts with sleep pressure (adenosine buildup from wakefulness) to determine when you feel sleepy.
What happens in the brain when you're sleep deprived?
Sleep deprivation impairs the prefrontal cortex (decision-making, impulse control) while amplifying amygdala reactivity (emotional responses), producing emotional volatility. Cognitive performance deteriorates: reaction time, attention, and working memory all degrade. After 17-19 hours awake, performance resembles being legally drunk. Chronic partial sleep deprivation accumulates ‘sleep debt’ with compounding consequences.
Does the amount of sleep you need change with age?
Yes significantly. Newborns sleep 14-17 hours per day; teenagers need 8-10 hours (and have a biologically delayed circadian phase, they naturally stay up late and sleep in); adults need 7-9 hours; older adults typically maintain 7-8 hours but sleep more lightly and wake more often. The common belief that older people need less sleep is largely incorrect, they get less, but not because they need less.
What is the glymphatic system and what does it have to do with sleep?
The glymphatic system is a waste clearance network in the brain that uses cerebrospinal fluid to flush out metabolic byproducts, including amyloid-beta and tau proteins associated with Alzheimer’s disease. It is primarily active during sleep, particularly slow-wave sleep. Chronic sleep deprivation may impair glymphatic clearance and contribute to the accumulation of these proteins.
How does light affect sleep?
Blue-wavelength light (from sunlight and screens) is the primary signal that resets the circadian clock. Exposure to blue light at night suppresses melatonin production and delays sleep onset. Bright light exposure in the morning advances the circadian phase. Dimming lights and limiting screen exposure in the evening improves sleep quality; morning bright light helps with consistent sleep timing.