In 1953, a graduate student named Eugene Aserinsky was trying to keep himself awake in the lab late at night by monitoring the slow eye movements researchers thought characterized sleep. His equipment malfunctioned - or seemed to.
The recordings showed rapid, darting eye movements in sleeping subjects that Aserinsky assumed were an artifact of broken equipment. They were not. He had discovered REM sleep, and with it, opened the modern scientific era of sleep research.
What followed over the next seven decades was a systematic dismantling of almost everything people believed about sleep. Sleep was not simply absence of wakefulness.
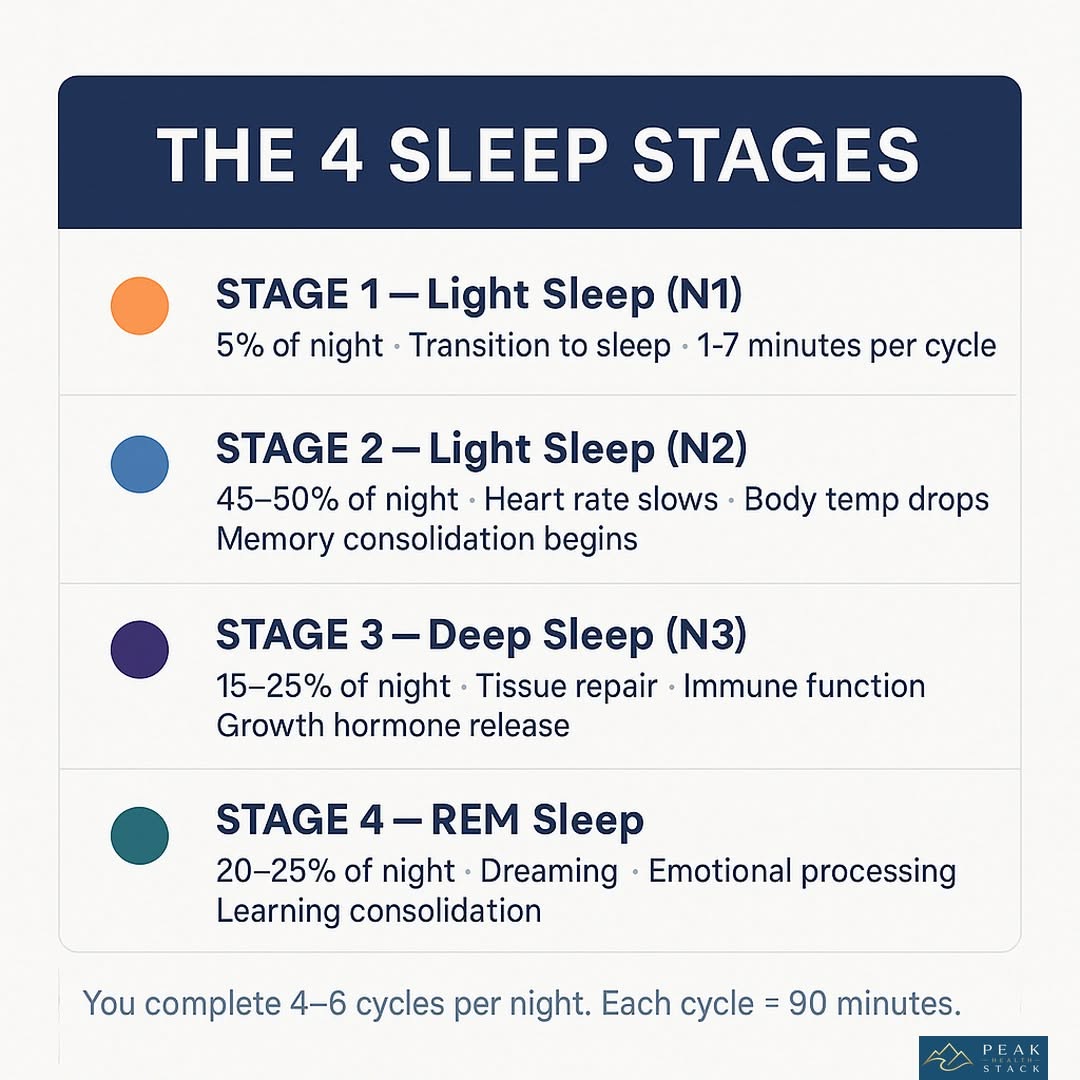
It was an active, staged, purposeful biological process with distinct architecture - cycling through four different stages roughly every 90 minutes, each with different neurological signatures and physiological functions.
Sleep was when memories consolidated, waste products were cleared from the brain, growth hormone was released, immune function peaked, and emotional experiences were processed and integrated.
The science of sleep and the science of sleep disruption are now among the most richly documented fields in medicine. Yet the practical gap between what sleep research has established and what most people know remains vast.
Most people with chronic sleep problems have tried some version of "trying harder to sleep" - an approach that generally makes insomnia worse - without ever encountering the treatment that works better than any medication for the long term.
That treatment is called Cognitive Behavioral Therapy for Insomnia. It is recommended as first-line treatment by the American College of Physicians, the American Academy of Sleep Medicine, and virtually every major sleep medicine organization worldwide. Most people have never heard of it.
"The shorter your sleep, the shorter your life span." - Matthew Walker, Why We Sleep (2017)
Key Definitions
Sleep architecture - The structure of sleep across a night, consisting of repeated 90-minute cycles. Each cycle contains NREM stages (N1 light sleep, N2 with sleep spindles, N3 deep slow-wave sleep) and REM sleep. Early cycles contain more slow-wave sleep; later cycles contain more REM.
Disrupting sleep duration or timing alters which stages are preferentially lost.
Circadian rhythm - The approximately 24-hour biological clock, orchestrated by the suprachiasmatic nucleus (SCN) in the hypothalamus, governing the timing of nearly all physiological processes: hormone release, body temperature, metabolism, and sleep propensity.
Primarily synchronized by light - specifically blue-wavelength light detected by intrinsically photosensitive retinal ganglion cells containing melanopsin.
Homeostatic sleep pressure (Process S) - The progressive build-up of sleep-promoting substances (primarily adenosine) during wakefulness. The longer you've been awake, the stronger the homeostatic drive to sleep.
This drive is distinct from the circadian drive - you can be sleepy (high Process S) but unable to sleep because the circadian clock is in its wrong phase.
Two-process model of sleep regulation - Borbely's framework describing sleep as determined by the interplay of homeostatic sleep pressure (Process S) and circadian rhythm (Process C). Optimal sleep occurs when both processes align: high homeostatic pressure meets a circadian signal permitting sleep onset.
Melatonin - A hormone secreted by the pineal gland in response to darkness, signaling the circadian clock that night has arrived. Does not cause sleep directly but shifts the timing of sleep propensity. Suppressed by light, particularly blue-wavelength light.
Sleep hygiene - The set of behavioral and environmental practices that promote sleep. Includes consistent sleep timing, cool and dark bedroom, avoidance of late caffeine and alcohol, and limiting pre-bed stimulation.
Necessary but often insufficient for chronic insomnia - it addresses precipitating and perpetuating factors but not the conditioned arousal that maintains chronic insomnia.
CBT-I (Cognitive Behavioral Therapy for Insomnia) - A structured psychological treatment for chronic insomnia addressing the thoughts, behaviors, and physiological arousal patterns that perpetuate sleeplessness.
Consists of sleep restriction, stimulus control, cognitive restructuring, relaxation training, and sleep hygiene. First-line treatment per clinical guidelines; produces more durable remission than pharmacotherapy.
Sleep restriction therapy - A component of CBT-I involving temporarily limiting time in bed to the actual hours slept, building homeostatic sleep pressure and consolidating fragmented sleep. Temporarily uncomfortable but highly effective.
Stimulus control - Reestablishing the psychological association between bed and sleep (not wakefulness, anxiety, or screen use). Involves using the bed only for sleep and sex, and leaving the bed when unable to sleep.
Chronotype - An individual's biological predisposition toward earlier or later sleep timing. Substantially genetic and age-dependent. "Owls" (evening types) have genuinely different circadian timing, not simply poor sleep habits or discipline.
Sleep efficiency - The proportion of time in bed actually spent sleeping. Normal sleep efficiency is 85-90%+. Spending 8 hours in bed while sleeping only 6 hours represents 75% efficiency - a marker of insomnia. Sleep restriction therapy raises sleep efficiency by reducing time in bed.
The Biology of Sleep Disruption
Before discussing solutions, understanding why sleep breaks down requires understanding the two systems that regulate it - and how they can work against you.
Sleep is controlled by the interaction of homeostatic sleep pressure (the longer you're awake, the sleepier you get) and the circadian clock (which independently promotes alertness and sleepiness at particular times of day).
When these systems align - when you're both homeostatically sleepy and in the circadian window for sleep - falling asleep is easy and sleep is consolidated.
Chronic insomnia almost always involves a third factor superimposed on this biological foundation: conditioned arousal. After nights of lying awake in bed, frustrated and anxious, the bed itself becomes a conditioned stimulus for wakefulness.
The arousal response - the cortisol spike, the racing thoughts, the physiological activation - becomes triggered by climbing into bed, regardless of how sleepy you felt five minutes earlier.
This is why the first intervention in CBT-I is not relaxation or medication. It is disrupting the conditioned association between bed and wakefulness. It is why people with chronic insomnia often sleep perfectly well in hotels, on sofas, or in any environment except their own bed - the conditioned arousal is bedroom-specific.
Understanding this mechanism transforms the approach to insomnia. The problem is not a deficiency in sleep drive or a broken biological clock (in most cases). It is a conditioned arousal pattern that has become self-perpetuating.
This is both better news (it can be extinguished) and worse news (it cannot be extinguished with sedating medication, which suppresses wakefulness without breaking the conditioned pattern).
What Doesn't Work (And Why People Keep Trying It)
Trying Harder to Sleep
The fundamental paradox of insomnia is that sleep is a passive process that cannot be forced. Increased effort at sleep - watching the clock, tensing muscles, willing yourself unconscious - increases cortisol, increases arousal, and makes sleep less likely.
This is the paradox of sleep effort, and it traps most people with chronic insomnia in an exhausting cycle.
Sleep specialists call this "sleep effort" - the active attempt to control sleep - and it is reliably associated with poorer sleep. The harder you try, the worse you sleep.
The therapeutic intervention is not to try harder but to do less: accept the wakefulness without catastrophizing, remove sleep-incompatible behaviors from the bedroom, and trust the homeostatic pressure to eventually produce sleep.
Sleeping In to Compensate
After a poor night's sleep, the instinct is to sleep later the following morning. This is counterproductive for chronic insomnia. Sleeping later reduces the homeostatic sleep pressure that would otherwise build through the day, making it harder to fall asleep the following night and perpetuating the cycle.
Consistent wake time - regardless of how poorly the previous night went - is one of the most powerful sleep stabilizers available. It anchors the circadian rhythm and ensures that homeostatic pressure is maximally built before the sleep window.
Spending More Time in Bed
Extending time in bed to "make up" for missed sleep is another intuitive but counterproductive response. More time in bed without more time asleep decreases sleep efficiency and deepens the conditioned association between bed and wakefulness.
A person spending 9 hours in bed while sleeping 6 is reinforcing the experience of lying awake in bed - exactly what needs to be broken.
Alcohol as a Sleep Aid
Roughly 20% of adults report using alcohol to help with sleep. Alcohol does accelerate sleep onset - it is sedating and reduces anxiety. But it severely impairs sleep architecture.
Alcohol is metabolized over several hours; as blood alcohol drops in the second half of the night, REM sleep rebounds intensely (after being suppressed in the first half), producing fragmented sleep, vivid or disturbing dreams, and early morning awakening.
The net effect is sleep that is lighter, more fragmented, and lacking in the restorative stages.
CBT-I: The Treatment That Works
Cognitive Behavioral Therapy for Insomnia is not a single technique but a structured set of evidence-based interventions, typically delivered over 6-8 sessions, addressing the multiple factors that maintain chronic insomnia.
Sleep Restriction
The counterintuitive core of CBT-I. If you're sleeping 5 hours per night while spending 8 hours in bed, your prescribed sleep window is initially 5 hours. You are allowed in bed only between (for example) 1am and 6am - regardless of how tired you are at 10pm.
This rapid sleep restriction rapidly builds homeostatic sleep pressure. By the second or third night, the accumulated adenosine drives powerfully consolidated, efficient sleep during the restricted window. As sleep efficiency rises above 85-90%, the window is extended by 15-30 minutes per week.
Sleep restriction is uncomfortable. You will be sleep-deprived in the first week. Most patients see significant improvement in 2-3 weeks; complete response within 6-8 weeks is typical.
Durable remission - continued improvement after treatment ends - is the norm, unlike with sleep medication, where insomnia typically returns upon discontinuation.
Stimulus Control
Restoring the bed's function as a cue for sleep rather than wakefulness:
- Use the bed only for sleep and sex
- If unable to sleep within approximately 20 minutes, leave the bed and do something calm in dim light until sleepy, then return
- Maintain a consistent wake time regardless of sleep quality
- Avoid naps (during the intensive phase of treatment)
These instructions feel wrong to sleep-deprived patients - "Why would I get out of bed when I'm exhausted?" - but they systematically disrupt the conditioned arousal pattern.
Each night of leaving the bed when awake and returning only when sleepy weakens the bed-wakefulness association and strengthens the bed-sleep association.
Cognitive Restructuring
Chronic insomnia is sustained by catastrophic thoughts about sleep:
- "I'll never sleep again"
- "I need 8 hours or I can't function"
- "Another night without sleep and I'll lose my job/health/sanity"
These thoughts increase arousal and make sleep impossible. Cognitive restructuring involves identifying these automatic thoughts and systematically challenging them with evidence. Most people function better than they fear on reduced sleep.
Most insomnia episodes do resolve. The next-day catastrophes people anticipate from poor sleep are almost always less severe than feared.
This is not positive thinking. It is more accurate thinking - replacing distorted catastrophizing with realistic appraisals that reduce the anxiety driving the conditioned arousal.
Relaxation Training
Progressive muscle relaxation, diaphragmatic breathing, and imagery-based relaxation can reduce the physiological arousal that maintains wakefulness. These techniques work by activating the parasympathetic nervous system, reducing cortisol, and providing an alternative focus to the ruminative worry that characterizes insomnia.
They are an adjunct to behavioral interventions, not a standalone treatment for chronic insomnia. Relaxation reduces arousal; it does not break the conditioned association between bed and wakefulness.
Light: The Most Powerful Lever on Your Sleep Timing
Light is the primary signal that synchronizes the circadian clock - and it is the most modifiable variable for most people struggling with sleep timing.
The mechanism: intrinsically photosensitive retinal ganglion cells in the eye contain a photopigment called melanopsin that is maximally sensitive to blue-wavelength light (~480nm). These cells project directly to the SCN and signal: daytime is happening.
In response, the SCN suppresses melatonin secretion and advances or delays the biological clock depending on when the light arrives.
Morning light exposure advances the circadian clock - shifting sleep propensity earlier. Even 10-15 minutes of outdoor light in the first hour after waking has measurable effects on circadian entrainment.
This is why morning light exposure is the single most evidence-supported intervention for people who struggle to fall asleep early enough or wake up at their desired time.
Evening blue light exposure delays the circadian clock - shifting sleep propensity later. Looking at bright screens in the 1-2 hours before bed suppresses melatonin and pushes the circadian signal for sleep onset later into the night.
Controlled studies show that smartphone and tablet use at night delays sleep onset by 30-60 minutes and reduces sleep quality, with effects measurable via polysomnography.
The practical protocol:
- Morning: seek bright light within 30-60 minutes of waking (outdoors is far more effective than indoor lighting)
- Evening: reduce overhead lighting intensity in the 1-2 hours before bed; use warm-spectrum bulbs or lamps; use blue-light filtering glasses or screen settings if screen use is unavoidable
- Night: the bedroom should be as dark as possible during sleep; even small amounts of ambient light during sleep reduce melatonin and sleep quality
For shift workers, jet lag, and people with delayed sleep phase disorder (the "extreme owl" whose biological clock is genuinely shifted later than desired), strategic light exposure and avoidance is the primary clinical intervention - more effective than any medication for realigning circadian timing.
Temperature: An Underrated Variable
Core body temperature must drop approximately 1-2�C (1.8-3.6�F) for sleep to initiate. This is not a consequence of sleep - it is a prerequisite. The body actively loses heat through peripheral vasodilation: blood flow to the hands and feet increases, and heat radiates away.
This is why warm hands and feet are associated with faster sleep onset.
Ambient room temperature dramatically affects this process:
| Bedroom Temperature | Effect on Sleep |
|---|---|
| Below 16�C (60�F) | May impair sleep for most people; too cold for thermoregulation |
| 18-20�C (65-68�F) | Optimal for most adults; facilitates core cooling |
| 23-25�C (73-77�F) | Increases wakefulness, reduces slow-wave sleep |
| Above 26�C (79�F) | Significantly impairs sleep architecture; increases restless sleep |
Research by Matthew Walker, Charles Czeisler, and others consistently identifies thermal environment as one of the most impactful modifiable sleep variables - more controllable for most people than noise, and whose importance is underappreciated.
Hot baths or showers 1-2 hours before bed paradoxically improve sleep onset. The mechanism is counterintuitive: the warm water causes peripheral vasodilation, accelerating heat loss from the skin. Core body temperature actually drops more rapidly after the bath than it would have without it.
The bath is a heat-dissipation mechanism, not a warming intervention.
Caffeine: A Half-Life Problem
Caffeine is the most widely consumed psychoactive substance on Earth and one of the most commonly underestimated sleep disruptors.
The mechanism: caffeine blocks adenosine receptors. Adenosine builds up during wakefulness as a byproduct of neural activity, progressively signaling "sleep pressure." Caffeine doesn't clear adenosine - it masks the signal.
When caffeine is eventually cleared, the accumulated adenosine, which has continued building throughout the caffeine block, rushes back in, producing the characteristic caffeine "crash."
The critical pharmacological fact is caffeine's half-life: 5-7 hours. This means:
- A coffee at 8am: approximately 12% of caffeine remains at midnight
- A coffee at noon: approximately 25-50% remains at midnight (depending on metabolism)
- A coffee at 2pm: approximately 33-50% remains at 9pm - precisely when you're trying to initiate sleep
The half-life is highly variable between individuals based on CYP1A2 enzyme genetics. Fast metabolizers clear caffeine quickly and are less affected by afternoon coffee; slow metabolizers retain caffeine much longer and may be significantly disrupted by any caffeine after noon.
Matthew Walker's research found that 400mg of caffeine consumed 6 hours before bed - despite subjective reports of normal sleep - reduced slow-wave sleep by 20% as measured by polysomnography. The subjects felt they slept normally; their brains were measurably less deeply asleep.
Walker described this as equivalent to aging 10-15 years in sleep quality, invisible to the drinker.
The practical guideline supported by the evidence: caffeine cutoff of 12:00-1:00pm for most people. Earlier for slow metabolizers or anyone who notices sleep disruption from afternoon caffeine.
Alcohol: What It Actually Does
Alcohol is perhaps the most counterproductive widespread sleep intervention. The logic seems sound - alcohol relaxes you, reduces anxiety, helps you fall asleep. The pharmacology is correct: alcohol is a GABA agonist and glutamate antagonist, meaning it sedates, reduces anxiety, and accelerates sleep onset.
But alcohol's effects on sleep architecture are severely negative:
First half of the night (while alcohol is being metabolized): REM sleep is suppressed. The sedating effects predominate; sleep seems deep.
Second half of the night (as blood alcohol drops): REM rebound - intense, fragmented REM sleep replaces what was suppressed. This produces vivid or disturbing dreams, lighter and more fragmented sleep, and early morning awakening as the rebound pushes the brain toward wakefulness.
Additional effects include: relaxation of upper airway muscles (worsening snoring and sleep apnea - alcohol-disrupted nights are often the worst nights for people with undiagnosed apnea); disruption of the normal body temperature regulation during sleep; increased urination from alcohol's diuretic effect causing nocturnal awakenings.
The net result: alcohol-assisted sleep is lighter, more fragmented, shorter, and significantly reduced in the REM sleep critical for emotional processing, memory consolidation, and mental health. This is not a small effect. Regular alcohol use before sleep, even moderate amounts, measurably reduces sleep quality across the full night.
Melatonin: What It Can and Cannot Do
Melatonin is the most widely sold sleep supplement and among the most misused. Understanding what it actually does - and does not do - prevents both over-reliance and dismissal.
What melatonin does: signals darkness to the circadian clock. The pineal gland releases melatonin as light fades; the SCN interprets this as "night is beginning." Melatonin tells the clock when night has arrived - it does not cause sleep. It shifts the timing of sleep propensity.
Where melatonin works well:
- Jet lag: taking melatonin at the destination bedtime helps shift the clock faster to the new timezone
- Shift work: for workers whose circadian timing must shift to match unusual schedules
- Delayed sleep phase syndrome: people whose biological clocks run genuinely late can use low-dose evening melatonin to advance sleep onset timing
- In older adults: melatonin secretion declines with age; supplementation may partially restore youthful timing
Where melatonin has weak evidence: general insomnia in people without circadian misalignment. If your insomnia involves difficulty falling asleep despite appropriate timing, or staying asleep, melatonin is unlikely to help significantly. The clock timing is not the problem.
The dose problem: commercial supplements typically contain 3-10mg. Physiological melatonin levels are orders of magnitude lower; 0.1-0.3mg is sufficient to produce a maximal clock-shifting signal. Higher doses do not improve efficacy and may cause daytime grogginess.
If melatonin is appropriate for your situation, 0.5mg taken 30-60 minutes before desired sleep onset is consistent with the evidence. The common 10mg doses are pharmacological curiosities with no demonstrated advantage over physiological doses.
Building a Sleep Environment
The bedroom environment substantially influences sleep quality through multiple channels:
Darkness: the bedroom should be genuinely dark - not dim-ish but light-blocking. Even small amounts of ambient light during sleep (streetlights through thin curtains, standby lights on electronics) suppress melatonin during sleep and increase arousal. Blackout curtains or a sleep mask produce measurably better sleep quality.
Temperature: as discussed, 18-20�C (65-68�F) for most adults. Consider breathable natural-fiber bedding that doesn't trap heat; humidity also matters, as very dry air can disrupt nasal breathing.
Noise: consistent background noise (white noise, fan sound) attenuates the disruptive effect of intermittent sounds more effectively than silence. The brain continues monitoring for novel sounds during sleep; consistent background noise reduces the salience of these sounds.
Noise machines work not by blocking sound but by reducing the signal-to-noise ratio.
The phone: the bedroom phone question is not merely behavioral. The phone in the bedroom creates multiple sleep disruptions: blue light exposure, notification sounds causing arousal, and the psychological availability of stimulating content (news, social media) at exactly the time the brain should be transitioning to sleep.
Charging the phone in another room removes the largest single behaviorally modifiable sleep disruptor most people have.
The CBT-I vs. Medication Question
The clinical comparison between CBT-I and pharmacological sleep treatment is one of the clearer outcomes in sleep medicine:
| Factor | CBT-I | Sleep Medication |
|---|---|---|
| Short-term efficacy | Comparable | Comparable |
| Long-term efficacy | Superior | Inferior (tolerance develops) |
| Effect on sleep architecture | Improves | Some stages suppressed |
| Risk of dependence | None | Yes (particularly benzodiazepines, Z-drugs) |
| Efficacy after treatment ends | Maintained or improved | Typically reverts |
| Side effects | Temporary sleep deprivation during restriction phase | Multiple; cognitive impairment, next-day sedation |
This comparison - CBT-I superior for long-term outcomes - has been demonstrated in multiple meta-analyses and forms the basis of the American College of Physicians' recommendation that CBT-I be used as first-line treatment for chronic insomnia disorder.
The practical barrier is access: CBT-I requires a trained therapist or a structured program, while medication requires only a prescription. Digital CBT-I programs (Sleepio, Somryst) have demonstrated efficacy approaching in-person therapy in randomized controlled trials and substantially expand access.
For related concepts, see what happens when you don't sleep, how sleep works, and how to improve your memory.
Sources & Further Reading
- Morin, C. M., et al. (2009). Cognitive Behavioral Therapy, Singly and Combined with Medication, for Persistent Insomnia. JAMA, 301(19), 2005-2015. DOI: 10.1001/jama.2009.681
- Qaseem, A., et al. (2016). Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline from the American College of Physicians. Annals of Internal Medicine, 165(2), 125-133. DOI: 10.7326/M15-2275
- Chang, A.-M., et al. (2015). Evening Use of Light-Emitting eReaders Negatively Affects Sleep, Circadian Timing, and Next-Morning Alertness. Proceedings of the National Academy of Sciences, 112(4), 1232-1237. DOI: 10.1073/pnas.1418490112
- Walker, M. P., Brakefield, T., Morgan, A., Hobson, J. A., & Stickgold, R. (2002). Practice with Sleep Makes Perfect: Sleep-Dependent Motor Skill Learning. Neuron, 35(1), 205-211. DOI: 10.1016/S0896-6273(02)00746-8
- Drake, C., et al. (2013). Caffeine Effects on Sleep Taken 0, 3, or 6 Hours before Going to Bed. Journal of Clinical Sleep Medicine, 9(11), 1195-1200. DOI: 10.5664/jcsm.3170
- Roehrs, T., & Roth, T. (2001). Sleep, Sleepiness, and Alcohol Use. Alcohol Research & Health, 25(2), 101-109.
- Borbely, A. A., & Achermann, P. (1999). Sleep Homeostasis and Models of Sleep Regulation. Journal of Biological Rhythms, 14(6), 557-568. DOI: 10.1177/074873099129000894
- Sloane, P. D., et al. (2007). High-Intensity Environmental Light in Dementia: Effect on Sleep and Activity. Journal of the American Geriatrics Society, 55(1), 15-22.
Health note: This article is general educational information about how a topic works, not medical, psychological, or mental-health advice, diagnosis, or treatment. Everyone's situation is different, and research findings describe groups, not individuals.
If you are struggling or have concerns about your health, please talk to a qualified professional such as a doctor or licensed therapist.
If you are in crisis or thinking about harming yourself, contact your local emergency services or a crisis line right away, in the US you can call or text 988 (Suicide & Crisis Lifeline); elsewhere, find local lines at findahelpline.com.
Frequently Asked Questions
What is CBT-I and why is it considered the first-line treatment for insomnia?
Cognitive Behavioral Therapy for Insomnia (CBT-I) is a structured psychological treatment addressing the thoughts, behaviors, and physiological arousal patterns that perpetuate chronic insomnia. It includes sleep restriction (temporarily limiting time in bed to consolidate sleep), stimulus control (reestablishing the association between bed and sleep), cognitive restructuring (challenging catastrophic thoughts about sleep), sleep hygiene education, and relaxation techniques. Meta-analyses show CBT-I outperforms sleep medication for long-term outcomes, medication works while taken but dependence and tolerance develop; CBT-I produces durable improvements. The American College of Physicians recommends CBT-I as the first-line treatment for chronic insomnia.
How does light exposure affect sleep?
Light is the primary zeitgeber (‘time-giver’) that synchronizes the circadian rhythm. Retinal melanopsin-containing cells detect blue-wavelength light (~480nm) and signal the suprachiasmatic nucleus (SCN) to suppress melatonin and advance or delay the biological clock. Morning bright light advances the clock (making you tired earlier); evening blue light delays it (pushing sleep onset later). Practical implications: morning light exposure (even 10-15 minutes outside) anchors the circadian rhythm; avoiding bright and blue-wavelength light in the 1-2 hours before bed reduces clock delay; phone and screen blue light at night delays sleep onset by 30-60 minutes in controlled studies.
What temperature should my bedroom be for optimal sleep?
Sleep onset requires core body temperature to drop approximately 1-2°C (1.8-3.6°F). This cooling occurs partly through peripheral vasodilation, you lose heat through hands and feet (why warm feet help you fall asleep faster). An ambient temperature that facilitates this cooling, approximately 65-68°F (18-20°C) for most adults, optimally supports sleep onset and sleep quality. Research by Czeisler, Walker, and others consistently identifies thermal environment as one of the most impactful modifiable sleep variables. Hot rooms suppress deep slow-wave sleep; the temperature drop in the early morning hours contributes to natural waking.
Does alcohol help or hurt sleep?
Alcohol impairs sleep quality despite helping sleep onset. Alcohol is a GABA agonist and glutamate antagonist, it sedates and reduces anxiety, which can accelerate sleep onset. However: alcohol suppresses REM sleep in the first half of the night; as alcohol is metabolized (typically in the second half of the night), REM rebounds intensely, producing vivid and disturbing dreams and fragmented sleep. Alcohol also relaxes upper airway muscles, worsening snoring and sleep apnea. The net effect: alcohol-assisted sleep is lighter, more fragmented, and lacking in the REM sleep critical for emotional processing and memory consolidation.
How does caffeine affect sleep?
Caffeine blocks adenosine receptors, delaying the subjective sense of sleepiness but not clearing the accumulated adenosine (which continues building). Caffeine’s half-life is 5-7 hours: a coffee at 2pm still has half its caffeine present at 7-9pm. This doesn’t mean you can’t fall asleep, but it does mean your sleep architecture is altered, with reduced slow-wave sleep even if subjective sleep quality seems normal. Walker’s research found afternoon caffeine reduced slow-wave sleep by 20%, equivalent to aging 10-15 years in sleep quality, without subjects noticing the reduction. A practical cut-off of 12-1pm for caffeine intake is supported by the half-life evidence.
What is sleep restriction therapy and how does it work?
Sleep restriction is a counterintuitive but highly effective component of CBT-I: temporarily limiting time in bed to the actual hours slept (e.g., if you sleep 5 hours but spend 8 in bed, your prescribed ‘sleep window’ is initially 5 hours). This severe sleep restriction rapidly builds homeostatic sleep pressure (adenosine accumulation), which consolidates fragmented sleep into a more solid block. As sleep efficiency (proportion of time in bed actually sleeping) improves above 85-90%, the window is gradually extended. Most patients see significant improvement within 1-3 weeks. Sleep restriction is temporarily uncomfortable, you will be sleep-deprived, but produces durable remission of insomnia.
Do sleep supplements like melatonin or magnesium actually work?
Melatonin’s evidence is limited and dose-specific. It is effective for circadian rhythm disorders (jet lag, shift work, delayed sleep phase syndrome), it signals darkness to the SCN and helps shift the clock timing. For general insomnia in people without circadian misalignment, evidence is modest at best. Most commercial supplements use doses (3-10mg) far above physiological levels (0.1-0.3mg is sufficient to shift the clock); lower doses may be as effective. Magnesium glycinate has some evidence for sleep quality improvement, likely through GABA receptor modulation and muscle relaxation. Valerian root evidence is consistently negative across rigorous trials. Prescription sleep medications work but carry dependence risk; CBT-I remains preferable for chronic insomnia.