Impact: When a combat veteran hears a car backfire and throws himself to the ground in a parking lot, his body has not failed to understand that he is in a supermarket parking lot. His body understands, at one level of processing, exactly where he is.
What has happened is that the car's sound has bypassed rational evaluation and activated a survival system that was correctly calibrated for a different environment, a system that still believes, at a cellular level, that life is under immediate threat.
Bessel van der Kolk, the Dutch-American psychiatrist who has spent four decades studying trauma, describes this as the body failing to understand that the danger is past.
The title of his 2014 book, "The Body Keeps the Score," refers to this central observation: traumatic experience does not merely leave psychological impressions. It leaves physical ones.
That book spent years on the New York Times bestseller list, selling millions of copies to readers who recognized themselves in its descriptions and found, often for the first time, a vocabulary for experiences that had previously felt unspeakable or shameful.
Its success reflected a gap: mainstream psychiatry had for decades framed trauma primarily as a cognitive and behavioral problem amenable to talking cures, while van der Kolk and colleagues like Peter Levine and Judith Herman were documenting how profoundly trauma rewired the body's nervous system in ways that verbal therapy alone often failed to address.
The field was catching up to what survivors already knew.
Today, trauma research sits at one of medicine's most fertile intersections. Neuroscience, psychiatry, immunology, epigenetics, and sociology all contribute to an understanding of how overwhelming experience reshapes biology.
The ACEs (Adverse Childhood Experiences) study, the most replicated finding in public health in the past 30 years, has demonstrated that childhood trauma has dose-response relationships with virtually every major chronic disease, from heart disease to cancer to autoimmune conditions.
Understanding what trauma is, how it works in the body, and what interventions actually help is not merely relevant to the approximately 20 percent of adults who will meet criteria for PTSD at some point. It is relevant to understanding human health broadly.
"Trauma is not the story of something that happened back then. It's the current imprint of that pain, horror, and fear living inside people." - Bessel van der Kolk, psychiatrist and trauma researcher, author of "The Body Keeps the Score"
Key Definitions
Trauma: An experience (or series of experiences) that overwhelms a person's capacity to cope, typically involving perceived threat to life or bodily integrity, helplessness, and intense fear, horror, or disgust. Note that trauma refers to the impact of the event on the individual, not to the event itself.
PTSD (Post-Traumatic Stress Disorder): A clinical diagnosis requiring four clusters of symptoms persisting more than one month following a traumatic event: intrusion (flashbacks, nightmares), avoidance (of reminders of the trauma), negative cognitions and mood, and hyperarousal (exaggerated startle, hypervigilance, sleep disturbance).
| Body System | Trauma Effect | Manifestation |
|---|---|---|
| Nervous system (ANS) | Dysregulation of sympathetic/parasympathetic balance | Chronic fight-or-flight; freeze states; difficulty regulating arousal |
| HPA axis | Altered cortisol rhythm; hyperreactive stress response | Exaggerated reactions to minor stressors |
| Immune system | Chronic low-grade inflammation | Higher rates of autoimmune conditions, slower healing |
| Gut-brain axis | Altered gut microbiome; increased gut permeability | IBS, digestive problems, mood dysregulation |
| Musculoskeletal | Chronic muscle tension, especially in neck, jaw, and pelvis | Chronic pain conditions, fibromyalgia-type symptoms |
Complex PTSD (C-PTSD): A condition resulting from prolonged, repeated trauma, particularly in childhood or contexts involving captivity or coercive control. In addition to PTSD symptoms, it involves emotional dysregulation, negative self-concept, and relational difficulties. Added to ICD-11 in 2018.
HPA axis: The hypothalamic-pituitary-adrenal axis, the body's primary stress-response system. Involves the hypothalamus releasing corticotropin-releasing hormone (CRH), which stimulates the pituitary to release ACTH, which stimulates the adrenal glands to produce cortisol. Dysregulated in PTSD.
Polyvagal theory: Stephen Porges' framework proposing three hierarchical states of the autonomic nervous system: social engagement (ventral vagal), fight-or-flight (sympathetic), and shutdown or freeze (dorsal vagal immobilization).
What Trauma Actually Is
The word "trauma" has been significantly expanded in popular usage, sometimes to the point where it risks becoming meaningless. People describe being "traumatized" by mildly unpleasant experiences, traffic jams, or social embarrassments.
Meanwhile, clinicians sometimes use definitions that are restrictively narrow, limiting the term to events involving direct physical threat in ways that exclude significant categories of psychological injury.
The DSM-5 defines qualifying traumatic events as exposure to actual or threatened death, serious injury, or sexual violence. This must occur through direct experience, witnessing the event, learning that it happened to a close person, or repeated or extreme exposure to aversive details (as in emergency responders).
This definition captures a great deal but deliberately excludes chronic emotional abuse, psychological coercion, and many forms of medical trauma that research suggests can produce PTSD-equivalent symptom profiles.
Judith Herman's clinical and theoretical framework, developed in "Trauma and Recovery" (1992) and still influential, emphasized that single-incident trauma, while serious, differs qualitatively from repeated, prolonged trauma occurring in relationships of captivity or dependency, including childhood abuse, domestic violence, and hostage situations.
Herman coined the term "complex post-traumatic stress disorder" to describe the sequelae of this latter category, which she argued the DSM's PTSD criteria failed to capture.
What unifies the diverse traumatic experiences is their effect on the nervous system. Traumatic events exceed the individual's existing coping resources, producing an experience of overwhelming helplessness.
The brain registers the event as incompletely processed, maintaining a state of physiological alarm that would normally resolve once the threat had passed.
This incomplete processing, rather than the severity of the event itself, is what determines whether someone develops lasting traumatic symptoms.
The Neurobiology: What Happens to the Brain
Rachel Yehuda, Professor of Psychiatry and Neuroscience at Mount Sinai in New York and one of the world's leading PTSD researchers, has spent her career documenting the neurobiological signature of trauma. Her research has established that PTSD involves lasting changes in three key brain structures and their interactions.
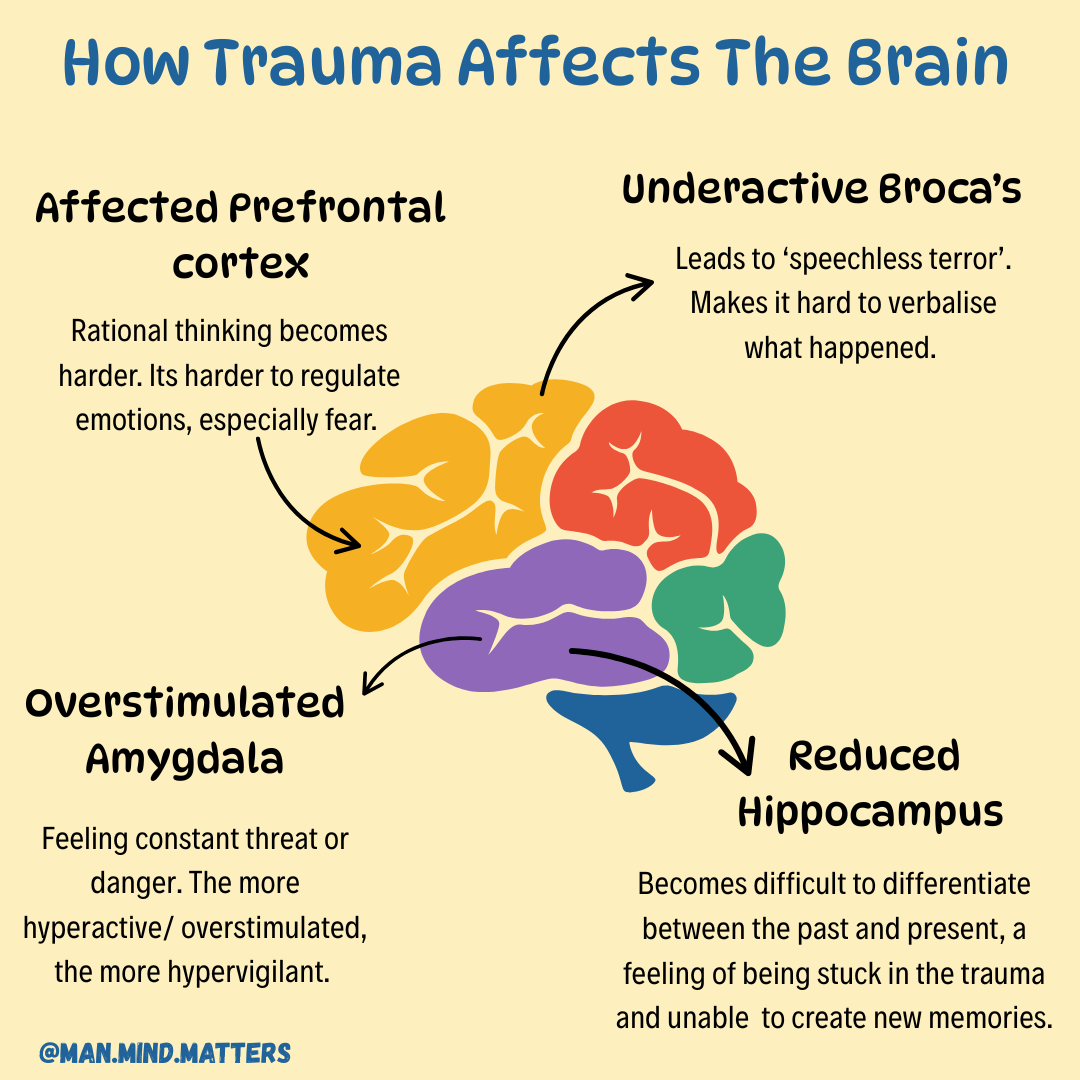
The amygdala, an almond-shaped structure deep in the temporal lobe that serves as the brain's threat-detection center, becomes hyperactive in PTSD.
It fires more readily in response to stimuli associated with the trauma, and, through generalization, in response to a widening circle of stimuli that bear any resemblance to the original threat.
This accounts for the hypervigilance characteristic of PTSD: the world is scanned constantly for danger, with false alarms firing regularly.
The prefrontal cortex (PFC), which provides contextual evaluation, emotional regulation, and the suppression of fear responses that are no longer appropriate, becomes suppressed.
When the amygdala fires a threat alarm, the PFC normally provides a reality check: yes, this sounds like a gunshot, but you are in a parking lot and there is no danger.
In PTSD, this PFC modulation is impaired. The alarm goes unchecked. This is why veterans in that parking lot cannot simply "think through" their response: the rational brain has been temporarily bypassed.
The hippocampus, critical for episodic memory and for establishing the temporal and spatial context of experiences, shows volume reduction in PTSD patients across multiple neuroimaging studies. This matters for two reasons.
First, the hippocampus normally provides the sense of temporal perspective that allows memories to be experienced as "in the past." When hippocampal function is compromised, traumatic memories can be re-experienced as present, which is the mechanism of the flashback.
Second, a smaller hippocampus impairs the discrimination between safe and dangerous situations, contributing to the generalization of fear responses.
Yehuda's research also documented a paradox that challenged the initial understanding of PTSD and cortisol. The expected finding was that people with PTSD would have elevated cortisol, reflecting a stuck-on stress response. Yehuda found the opposite: low cortisol, combined with high sensitivity to cortisol's effects.
The HPA axis in PTSD is not hyperactive in the way first assumed but is dysregulated in a complex way that involves enhanced negative feedback, meaning the system suppresses itself more aggressively in response to any cortisol release.
This dysregulation affects immune function, inflammation, and metabolic processes, contributing to the physical health consequences of trauma.
The ACEs Study: Trauma as a Public Health Crisis
The Adverse Childhood Experiences (ACEs) study is perhaps the most consequential epidemiological research in public health of the past three decades.
Conducted by Vincent Felitti at Kaiser Permanente in San Diego and Robert Anda at the CDC, the study enrolled over 17,000 adults receiving comprehensive physical examinations between 1995 and 1997 and asked them retrospectively about ten categories of childhood adversity: physical, emotional, and sexual abuse; physical and emotional neglect; household substance abuse; household mental illness; domestic violence; parental separation or divorce; and incarceration of a household member.
The results, published in 1998 in the American Journal of Preventive Medicine, were striking and have been replicated in multiple large national surveys since. ACEs were highly prevalent: 52 percent of participants reported at least one ACE, and 6.2 percent reported four or more.
ACEs were strongly correlated with each other, so that having one ACE significantly predicted having others. And ACEs showed a remarkably consistent dose-response relationship with virtually every major cause of adult morbidity and mortality.
Compared to people with no ACEs, individuals with four or more ACEs had: 2.4 times the lifetime risk of heart disease, 1.9 times the risk of cancer, 4.5 times the risk of depression, 12 times the risk of suicide attempts, 7.4 times the risk of alcoholism, and 10 times the risk of injection drug use.
The physical health findings were the most surprising to the medical establishment: that childhood emotional experiences had measurable relationships with adult cardiovascular disease and cancer decades later.
The mechanisms involve chronic HPA axis dysregulation, persistent inflammation, behavioral risk factors adopted as coping strategies, and potentially epigenetic changes.
The ACEs study has been central to the trauma-informed care movement, which argues that healthcare, education, and social services should be organized around understanding that a substantial proportion of the people they serve have histories of significant trauma, and that this history is causally relevant to their current presentations.
The movement has transformed policies in pediatrics, child welfare, and primary care.
Polyvagal Theory: Porges and the Social Nervous System
Stephen Porges, Distinguished University Scientist at Indiana University and research professor of psychiatry at the University of North Carolina at Chapel Hill, published polyvagal theory in the 1990s and developed it through subsequent decades.
The theory has become enormously influential in trauma therapy, though some of its specific anatomical claims have been contested by neuroanatomists.
Porges proposed that the autonomic nervous system is not simply a two-branch system (sympathetic fight-or-flight versus parasympathetic rest-and-digest) but has three hierarchical states, each representing an evolutionary layer.
The most evolutionarily ancient is the dorsal vagal system, shared with primitive vertebrates, which produces immobilization, shutdown, and dissociation when threat is overwhelming. The sympathetic system mobilizes for active defense through fight or flight.
The most evolutionarily recent is the ventral vagal system, unique to mammals, which supports social engagement: calm interaction, co-regulation with others, facial expressiveness, and the integrated functioning of the face, voice, heart, and respiration.
In Porges' model, traumatic threat first activates the sympathetic system. If active defense is impossible (as in child abuse by a caregiver, or captivity), the dorsal vagal system takes over, producing the freeze or collapse response.
Many trauma survivors describe the dissociation, emotional numbness, and sense of detachment during overwhelming events as this dorsal vagal shutdown.
Recovery from trauma involves, in polyvagal terms, moving back up the hierarchy from shutdown to mobilization to social engagement, restoring the capacity for safe connection with others.
The theory has been criticized by neuroscientists including Peter Goadsby and others who point out that polyvagal theory misattributes some functions to specific vagal pathways in ways not fully supported by the anatomical literature. Porges has responded to these criticisms.
The clinical utility of the framework is generally accepted even by some who question its precise neuroanatomical claims, because it provides therapists with a practical model for understanding trauma responses that informs interventions effectively.
The Body Keeps the Score: Somatic Dimensions of Trauma
Bessel van der Kolk's central contribution to trauma research has been the systematic documentation that trauma is stored in the body, not merely in explicit narrative memory.
His research, conducted at the Trauma Center he founded in Brookline, Massachusetts, showed that traumatic memories are encoded differently from ordinary memories: they tend to be stored as fragmented sensory impressions (images, smells, sounds, physical sensations) rather than coherent narratives with temporal sequence and contextual framing.
This means that standard talk therapy, which asks patients to narrate their experiences, often cannot access the traumatically encoded material, which does not reside in narrative language.
Van der Kolk has argued that effective trauma treatment must address the body directly, through modalities including yoga, somatic therapies, EMDR, and rhythmic movement, rather than relying solely on verbal processing.
His research found that trauma survivors often show chronic patterns of somatic dysregulation: elevated resting muscle tension, abnormal heart rate variability, altered pain processing, and dysregulated arousal states. These somatic symptoms are not psychosomatic in the dismissive sense.
They reflect real physiological changes in the nervous system that result from the reorganization of threat-response circuits around a traumatic experience.
Epigenetic Transmission of Trauma
Rachel Yehuda's research on the children of Holocaust survivors added a disturbing dimension to trauma biology: the suggestion that trauma effects can be transmitted across generations through epigenetic mechanisms.
In studies published from the early 2000s onward, Yehuda found that children of Holocaust survivors had altered HPA axis profiles compared to demographically similar controls, including lower cortisol levels, heightened cortisol sensitivity, and higher rates of anxiety and PTSD in response to subsequent stressors.
Her 2016 paper in Biological Psychiatry reported epigenetic changes at a specific site on the glucocorticoid receptor gene (FKBP5) in Holocaust survivors and their children that were not found in unexposed controls or their children.
These methylation differences suggested that stress-induced epigenetic changes in the parent generation were transmitted to offspring, altering their physiological stress response systems without any direct exposure to the original trauma.
This research is preliminary, contested, and difficult to interpret. Critics point out methodological challenges including small sample sizes, potential confounding by shared environment, and the difficulty of distinguishing prenatal effects (maternal stress during pregnancy) from truly epigenetic transgenerational transmission.
Yehuda acknowledges these limitations while arguing that the biological plausibility of the mechanism, given what is known about epigenetic inheritance in animals, makes the findings worth pursuing. The field remains active.
What Treatments Actually Work
The evidence base for trauma treatments is unusually well-developed by psychiatric standards, driven partly by the military's investment in PTSD treatment research following the Vietnam and Gulf wars.
EMDR (Eye Movement Desensitization and Reprocessing), developed by Francine Shapiro in the late 1980s, involves having patients recall traumatic memories while simultaneously engaging in bilateral sensory stimulation, typically eye movements tracking the therapist's finger.
The World Health Organization recommends EMDR as a first-line treatment for PTSD. A 2020 meta-analysis by Chen and colleagues found large effect sizes (Hedges' g = 1.01) for EMDR compared to control conditions.
The mechanism of action remains debated: competing hypotheses include working memory interference, facilitated integration of traumatic memories, and REM sleep simulation.
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), which combines elements of exposure therapy, cognitive restructuring, and psychoeducation, is the most extensively studied psychological treatment for childhood trauma and has strong evidence in adult PTSD as well.
It involves gradual, structured exposure to trauma memories in a safe context, facilitating the processing and contextual embedding of memories that trauma impedes.
Prolonged Exposure (PE), developed by Edna Foa at the University of Pennsylvania, involves prolonged imaginal exposure to trauma memories and in-vivo exposure to feared but safe situations. Multiple randomized trials have shown PE effective, with response rates of approximately 60 to 80 percent.
It is more demanding than some alternatives and has higher dropout rates, but its efficacy for PTSD is among the most thoroughly documented.
Somatic therapies including Somatic Experiencing (developed by Peter Levine), sensorimotor psychotherapy (Pat Ogden), and body-based yoga interventions have growing evidence bases.
A 2014 study by van der Kolk and colleagues found that yoga significantly reduced PTSD symptoms compared to a control condition in women who had not responded adequately to other treatments.
These approaches directly address the somatic dimension of trauma that van der Kolk and Levine have argued is underaddressed by verbal therapies alone.
MDMA-assisted psychotherapy is in Phase 3 clinical trials through MAPS (Multidisciplinary Association for Psychedelic Studies) with promising results.
A 2021 Nature Medicine paper reported that 67 percent of participants in the MDMA group no longer met PTSD diagnostic criteria after three sessions, compared to 32 percent in the placebo group, with large effect sizes.
Practical Takeaways
Trauma is not weakness, character deficiency, or poor coping. It is a biological response to overwhelming experience that reorganizes the nervous system in lasting ways. Understanding this reduces self-blame and increases the likelihood of seeking effective help.
Physical symptoms, including chronic pain, gastrointestinal problems, autoimmune conditions, and cardiovascular disease, can be downstream consequences of trauma through HPA axis dysregulation and chronic inflammation. Trauma history is clinically relevant to physical health.
Effective treatments exist. EMDR and trauma-focused CBT have the strongest evidence, but the right treatment depends on the person, the trauma type, and the available resources. Somatic approaches may be necessary when verbal processing alone is insufficient.
Complex PTSD, resulting from childhood or prolonged interpersonal trauma, is different from single-incident PTSD and may require longer-term relational therapy in addition to trauma-focused techniques.
Childhood adversity assessed through ACEs screening has predictive value for adult health outcomes and is increasingly used in clinical settings as a routine element of health assessment.
For related reading, see What Causes Anxiety, How Stress Damages the Body, and How Epigenetics Works.
Sources & Further Reading
van der Kolk BA. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Viking; 2014.
Herman JL. Trauma and Recovery: The Aftermath of Violence. Basic Books; 1992.
Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine. 1998;14(4):245-258.
Yehuda R, Daskalakis NP, Bierer LM, et al. Holocaust exposure induced intergenerational effects on FKBP5 methylation. Biological Psychiatry. 2016;80(5):372-380.
Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. International Journal of Psychophysiology. 2001;42(2):123-146.
Chen YR, Hung KW, Tsai JC, et al. Efficacy of eye-movement desensitization and reprocessing for patients with posttraumatic-stress disorder: a meta-analysis of randomized controlled trials. PLoS ONE. 2014;9(8):e103676.
Mitchell JM, Bogenschutz M, Lilienstein A, et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine. 2021;27(6):1025-1033.
van der Kolk BA, Stone L, West J, et al. Yoga as an adjunctive treatment for posttraumatic stress disorder: a randomized controlled trial. Journal of Clinical Psychiatry. 2014;75(6):e559-e565.
Foa EB, Hembree EA, Rothbaum BO. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. Oxford University Press; 2007.
World Health Organization. Guidelines for the Management of Conditions Specifically Related to Stress. WHO; 2013.
Levine PA. Waking the Tiger: Healing Trauma. North Atlantic Books; 1997.
Maercker A, Cloitre M, Bachem R, et al. Complex post-traumatic stress disorder. Lancet. 2022;400(10347):60-72.
Health note: This article is general educational information about how a topic works, not medical, psychological, or mental-health advice, diagnosis, or treatment. Everyone's situation is different, and research findings describe groups, not individuals.
If you are struggling or have concerns about your health, please talk to a qualified professional such as a doctor or licensed therapist.
If you are in crisis or thinking about harming yourself, contact your local emergency services or a crisis line right away, in the US you can call or text 988 (Suicide & Crisis Lifeline); elsewhere, find local lines at findahelpline.com.
Frequently Asked Questions
What is the difference between trauma and PTSD?
Trauma refers to the experience of events that overwhelm a person’s capacity to cope and are perceived as threatening to life or integrity. PTSD (post-traumatic stress disorder) is a specific clinical diagnosis that requires particular symptoms, including intrusion, avoidance, negative cognitions and mood, and hyperarousal, persisting for more than a month and causing significant impairment. Many people experience trauma without developing diagnosable PTSD.
How does trauma change the brain?
Trauma dysregulates the stress-response system, producing lasting changes in the amygdala (which becomes hyperreactive, detecting threat everywhere), the prefrontal cortex (which becomes suppressed, reducing rational thinking and emotional regulation), and the hippocampus (which shrinks, impairing memory consolidation and context discrimination). Rachel Yehuda’s research at Mount Sinai has documented these neurobiological changes and their persistence long after the traumatic event.
What is complex PTSD and how is it different from PTSD?
Complex PTSD (C-PTSD) results from prolonged, repeated trauma, particularly interpersonal violence occurring in childhood or situations of captivity or coercive control. Judith Herman first described the condition in 1992. In addition to standard PTSD symptoms, C-PTSD involves emotional dysregulation, negative self-concept, and difficulties in relationships. It was officially added to ICD-11 in 2018 but is not yet in DSM-5.
What trauma treatments have the best evidence?
EMDR (Eye Movement Desensitization and Reprocessing) and trauma-focused cognitive behavioral therapy (TF-CBT) have the strongest evidence base. The WHO recommends EMDR and CBT as first-line treatments for PTSD. Prolonged Exposure therapy and Cognitive Processing Therapy are also well-evidenced. Somatic therapies including Somatic Experiencing and sensorimotor psychotherapy have growing evidence bases. MDMA-assisted psychotherapy is in Phase 3 clinical trials.
Can trauma be passed down through generations?
Research on epigenetic transmission of trauma, particularly Rachel Yehuda’s studies of Holocaust survivor descendants, suggests that trauma effects can be transmitted across generations through epigenetic mechanisms, not through changes in DNA sequence but through methylation patterns affecting gene expression. Children of Holocaust survivors show altered cortisol profiles similar to their parents. This is an active and somewhat contested area of research.
What is the polyvagal theory and does it hold up?
Polyvagal theory, developed by Stephen Porges at Indiana University, proposes that the autonomic nervous system has three hierarchical states: social engagement (ventral vagal), fight-or-flight (sympathetic), and shutdown or freeze (dorsal vagal). The theory has been widely adopted in trauma therapy. Some aspects of the underlying neuroscience are contested by researchers, but the clinical framework it provides for understanding trauma responses is considered valuable by many trauma clinicians.
How do you know if you have unresolved trauma?
Signs of unresolved trauma include persistent hypervigilance or startle responses, emotional numbness or disconnection, intrusive memories or flashbacks, difficulty with trust or intimacy, chronic physical tension, unexplained bodily symptoms, avoidance of reminders of past events, and difficulty tolerating strong emotions. These experiences exist on a spectrum and do not require a formal diagnosis to warrant seeking professional support.