Science: In 1980, the American Psychiatric Association published the third edition of its Diagnostic and Statistical Manual of Mental Disorders - DSM-III - and for the first time in the history of organized psychiatry, it formally acknowledged that external events, not just internal weakness or constitutional defect, could cause lasting mental illness in previously healthy people.
The new diagnosis was post-traumatic stress disorder, and its inclusion was the product of nearly a decade of advocacy by two groups who had until then been treated by the medical establishment as largely separate problems: Vietnam veterans, predominantly young men returning from a war whose legitimacy was in profound dispute, and survivors of sexual assault and domestic violence, predominantly women who had been systematically disbelieved and blamed by the institutions meant to help them.
The diagnosis had in fact a much longer history under other names. "Shell shock" was the British Army's informal term for the neurological and psychological symptoms observed in soldiers who had been exposed to artillery bombardment in World War I - the trench warfare that produced a generation of men who shook uncontrollably, relived their experiences in nightmares, could not speak, and were unable to return to the front.
The military establishment of the time vacillated between treating these men as casualties of genuine neurological injury and treating them as cowards engaged in malingering.
W.H.R. Rivers at Craiglockhart War Hospital used early talking-cure techniques with his patients, including the poet Siegfried Sassoon, and observed that the systematic re-exposure to traumatic memories, conducted within a therapeutic relationship, reduced symptoms.
This approach foreshadowed elements of what would later become prolonged exposure therapy.
World War II brought "combat fatigue" or "battle exhaustion" as the diagnostic terms, and psychiatrist Abram Kardiner's 1941 book "The Traumatic Neuroses of War" provided the most sophisticated prewar attempt at a systematic clinical description of what combat trauma did to the human nervous system.
Kardiner identified a syndrome he called "physioneurosis" - a persistent alteration of the nervous system's reactivity that could not be reduced to either pure psychology or pure physiology.
He was describing, in the language of his time, what neurobiological research would later characterize as a persistent alteration of the fear conditioning system.
"Traumatic events call into question basic human relationships. They breach the attachments of family, friendship, love, and community. They shatter the construction of the self that is formed and sustained in relation to others." - Judith Herman, Trauma and Recovery (1992)
Key Definitions
Post-traumatic stress disorder (PTSD): a psychiatric disorder that can develop following exposure to a traumatic event involving actual or threatened death, serious injury, or sexual violence, characterized by intrusion, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity persisting for more than one month and causing significant distress or functional impairment.
Criterion A: the DSM-5 definition of traumatic event exposure - the precipitating event must involve actual or threatened death, serious injury, or sexual violence, experienced directly, witnessed, learned about as happening to a close person, or through repeated/extreme exposure to aversive details.
| PTSD Symptom Cluster | Examples | Neurobiological Basis |
|---|---|---|
| Intrusion | Flashbacks, nightmares, intrusive memories | Amygdala over-encoding of fear memory; hippocampal fragmentation |
| Avoidance | Avoiding trauma reminders, emotional numbing | Behavioral suppression to prevent fear activation |
| Negative cognitions/mood | Distorted blame, persistent negative emotions, detachment | Prefrontal hypoactivity; disrupted memory contextualization |
| Hyperarousal | Hypervigilance, exaggerated startle, sleep disturbance | HPA-axis dysregulation; elevated norepinephrine |
Intrusion symptoms: involuntary re-experiencing of the traumatic event, including flashbacks (feeling as if the event is happening again), nightmares, and intense psychological or physiological distress when exposed to cues that resemble the event.
Hyperarousal: a persistent state of heightened alertness and reactivity, including exaggerated startle response, hypervigilance, sleep disturbance, irritability/angry outbursts, reckless behavior, and concentration difficulties.
Fear conditioning: the process by which a neutral stimulus acquires the capacity to trigger fear responses by being paired with a threatening stimulus; the fundamental learning mechanism underlying PTSD.
Fear extinction: the process by which conditioned fear responses are reduced when the conditioned stimulus is repeatedly presented without the threatening stimulus; impaired in PTSD.
HPA axis: hypothalamic-pituitary-adrenal axis; the neuroendocrine system regulating cortisol release in response to stress; dysregulated in PTSD in a characteristically paradoxical direction (low cortisol with hypersensitive feedback suppression).
Peritraumatic dissociation: a feeling of unreality, depersonalization, or emotional detachment during a traumatic event; one of the strongest prospective predictors of subsequent PTSD.
Prolonged Exposure (PE): a gold-standard cognitive-behavioral treatment for PTSD developed by Edna Foa, involving both imaginal and in vivo exposure to trauma reminders.
Cognitive Processing Therapy (CPT): a gold-standard cognitive-behavioral treatment for PTSD developed by Patricia Resick, targeting distorted beliefs ("stuck points") about the trauma and its meaning.
EMDR: Eye Movement Desensitization and Reprocessing; a trauma treatment developed by Francine Shapiro involving focus on traumatic memories while engaging in bilateral sensory stimulation.
Complex PTSD (C-PTSD): a diagnosis introduced in ICD-11 for PTSD developing from prolonged, repeated trauma, characterized by disturbances in affect regulation, self-concept, and interpersonal functioning beyond standard PTSD.
Moral injury: harm to a person's moral foundations from perpetrating, witnessing, or failing to prevent actions that violate deeply held moral beliefs; conceptually distinct from PTSD though often co-occurring.
The 1980 Breakthrough: Naming the Condition
The politics of the DSM-III's inclusion of PTSD are inseparable from the social and political context of the 1970s.
The Vietnam Veterans Against the War organized in 1967 and by the early 1970s were explicitly seeking psychiatric recognition for what their members were experiencing - not to claim disability benefits, though that was part of it, but to establish that they had been genuinely harmed by what they had been sent to do and had seen done.
Psychiatrists associated with the anti-war movement, particularly Robert Jay Lifton and Chaim Shatan, conducted "rap groups" with veterans and documented the symptom patterns they observed.
Simultaneously, the feminist movement was organizing around the recognition that sexual assault and domestic violence caused lasting psychological harm, and that this harm had been systematically dismissed by mental health professionals who attributed it to pre-existing weakness, neurosis, or even provocation.
The work of Ann Burgess and Lynda Holmstrom on "rape trauma syndrome," published in the American Journal of Psychiatry in 1974, was among the first systematic clinical descriptions of post-assault psychological responses.
These two advocacy efforts - from veterans and from feminist activists - converged in the DSM-III process and succeeded in inserting a new diagnosis.
The shared logic was powerful: different types of trauma produced recognizably similar symptom patterns, and the patterns were caused by the external events, not by pre-existing vulnerabilities.
The inclusion of PTSD in DSM-III was genuinely transformative. It established the principle that external events could cause lasting biological changes in the brain - a principle that most psychiatrists at the time still found conceptually difficult.
It opened funding streams for research on trauma. It established legal and policy frameworks for recognizing trauma-related disability. And it gave clinicians and patients a common vocabulary for experiences that had previously been either invisible or pathologized as personal weakness.
The Neuroscience of Fear Memory
PTSD is best understood neurobiologically as a disorder of fear memory - specifically, a failure of the normal processes by which fear memories are contextualized, modulated, and extinguished over time.
Fear Conditioning and the Amygdala
The basic neuroscience begins with Pavlovian fear conditioning, the process by which a previously neutral stimulus (a tone, a smell, a visual cue) acquires the capacity to trigger fear responses by being repeatedly paired with an inherently threatening unconditioned stimulus (electric shock, in standard animal studies).
After conditioning, the conditioned stimulus alone produces conditioned fear responses: freezing behavior, elevated heart rate, stress hormone release.
This process depends critically on the basolateral amygdala, a subcortical structure that detects threat signals and coordinates autonomic and behavioral fear responses.
In normal circumstances, conditioned fear responses are regulated by two other brain systems. The hippocampus provides contextual information: it encodes the spatial and temporal context in which the fear conditioning occurred, allowing the amygdala's response to be gated by context.
Fear responses appropriate in the dangerous context (a war zone, an assailant's apartment) should not be triggered in safe contexts (a supermarket, a therapy office).
The prefrontal cortex - particularly the ventromedial prefrontal cortex - provides top-down inhibitory control over amygdala responses, enabling fear extinction (the learned suppression of conditioned fear when the conditioned stimulus is repeatedly encountered in the absence of the threatening unconditioned stimulus).
In PTSD, both of these regulatory systems appear to be impaired. Fear responses are triggered by cues that merely resemble the original trauma regardless of the current safety of the context - a car backfiring triggers a combat veteran's full physiological terror response in a parking lot.
The prefrontal cortex fails to inhibit the amygdala's response. Extinction is impaired: the normal process of repeated safe exposure reducing fear responds is slower and less complete in people with PTSD. The result is persistent, context-inappropriate fear responses that resist normal learning.
The HPA Axis Paradox: Rachel Yehuda's Research
A puzzle that occupied researchers for decades was why the cortisol patterns in PTSD patients were paradoxical. The standard model of stress responses predicted elevated cortisol; many studies of individuals with chronic stress, depression, and exposure to acute stressors found elevated cortisol.
But Rachel Yehuda's research at the Bronx Veterans Affairs Medical Center and Mount Sinai School of Medicine found consistently low cortisol levels in Vietnam veterans with PTSD, with enhanced negative feedback suppression by dexamethasone.
Yehuda's interpretation was that PTSD does not involve a chronically activated stress response but rather a hypersensitive HPA axis that over-suppresses cortisol.
This distinction has significant implications: if PTSD represents a failure of the stress system to turn off rather than failure to mount a response, then the long-term sequelae of the condition - including heightened sensitization to subsequent stressors - make different biological sense.
The cortisol findings have been replicated across multiple trauma populations, including Holocaust survivors and their offspring, where Yehuda's research also found altered cortisol patterns in children of PTSD survivors, suggesting epigenetic transmission of stress response dysregulation.
Hippocampal Volume and the Chicken-and-Egg Problem
Multiple structural neuroimaging studies have found smaller hippocampal volumes in individuals with PTSD compared to both trauma-exposed controls without PTSD and healthy non-exposed controls.
The Bremner group at Yale reported approximately 8% smaller hippocampal volume in Vietnam veterans with PTSD; subsequent meta-analyses confirmed this finding across multiple trauma populations.
The critical interpretive question is whether reduced hippocampal volume is a consequence of trauma and PTSD (consistent with animal studies showing that severe chronic stress causes hippocampal neuronal death via glucocorticoid toxicity) or a pre-existing vulnerability that predisposes individuals to developing PTSD after trauma.
Landmark research by Mark Gilbertson and colleagues, examining hippocampal volume in identical twins where only one twin had been deployed to Vietnam, found that the non-PTSD twin of a PTSD-affected pair had smaller hippocampi than the non-PTSD twin of a non-PTSD-affected pair - consistent with pre-existing reduced hippocampal volume being a vulnerability factor rather than a consequence of trauma.
The debate about direction of causation is ongoing, and both effects may contribute.
Epidemiology: Who Gets PTSD
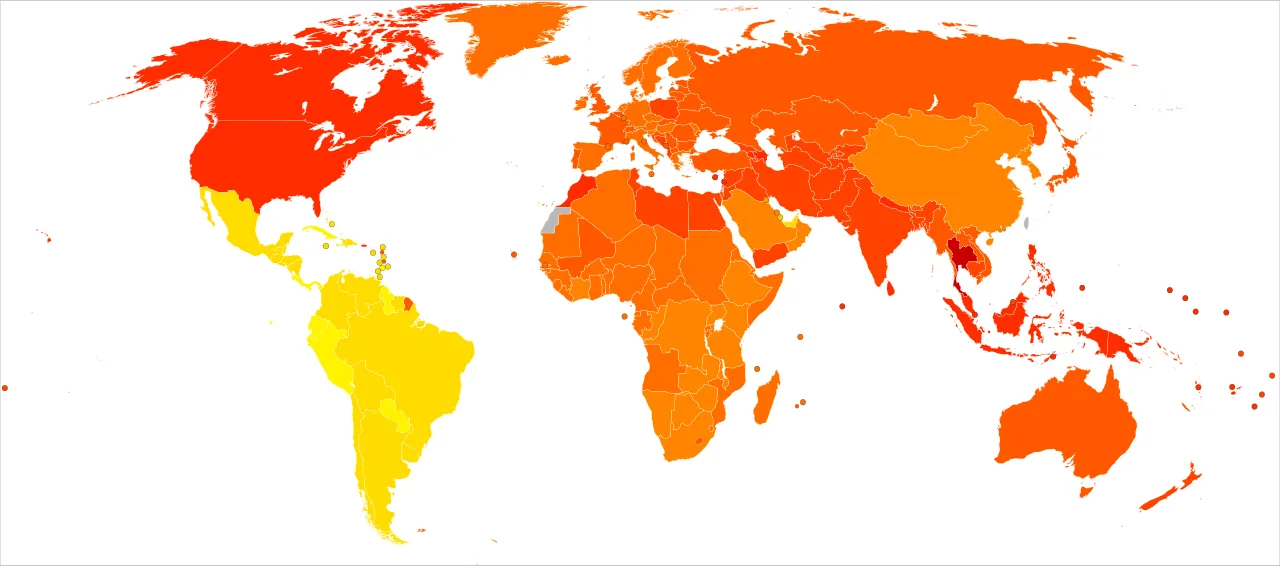
Lifetime prevalence of PTSD in the United States is approximately 7-8% of the general population, based on data from the National Comorbidity Survey and its replications. This masks substantial variation by trauma type and demographic group.
Among combat veterans deployed to Vietnam, Iraq, and Afghanistan, PTSD prevalence rates range from 15-30% in various studies, with methodological variation accounting for part of the range. Among survivors of sexual assault, conditional PTSD risk estimates range from 45-65%.
Motor vehicle accident survivors face approximately 20-30% conditional risk; natural disaster survivors approximately 15-20%.
Women develop PTSD at approximately twice the rate of men after controlling for trauma type - a finding consistent across cultures and study methodologies. The mechanisms are debated. Women are more likely to experience sexual assault, which carries the highest conditional PTSD risk of any trauma type.
There are also possible sex differences in cortisol reactivity, fear extinction efficiency, and the social response to trauma disclosure.
Trauma disclosure and social support after trauma are among the most robust protective factors; social support that involves believing the survivor, not blaming them, and providing practical assistance reduces PTSD risk substantially.
Evidence-Based Treatments
Prolonged Exposure Therapy
Prolonged Exposure (PE), developed by Edna Foa and colleagues at the University of Pennsylvania (and later the Center for the Treatment and Study of Anxiety at Penn), is derived from emotional processing theory - the principle that PTSD is maintained by pathological fear structures that prevent natural processing of the traumatic memory, and that these structures can be corrected through systematic, repeated engagement with feared stimuli in a safe therapeutic context.
PE consists of two primary components. In imaginal exposure, the patient repeatedly narrates the traumatic memory in the present tense for extended periods within session, with the therapist present to provide emotional support and to process the experience afterward.
The theory is that repeated engagement with the memory reduces its emotional charge through habituation and allows corrective learning: the memory can be held without catastrophe.
In vivo exposure involves constructing a hierarchy of avoided situations that are trauma-related but objectively safe (the location of the trauma, certain smells or sounds that trigger responses) and systematically approaching them rather than avoiding them.
Multiple RCTs demonstrate large effect sizes for PE, and it has been designated a gold-standard treatment by the VA/DoD Clinical Practice Guidelines and the American Psychological Association.
Meta-analyses find that approximately 80-90% of patients who complete PE show significant improvement, though drop-out rates are higher than in some less intense therapies.
Cognitive Processing Therapy
Cognitive Processing Therapy (CPT), developed by Patricia Resick and colleagues originally for rape survivors and subsequently validated across trauma populations, targets the cognitive distortions - "stuck points" - that maintain PTSD.
These stuck points are typically beliefs about the trauma and its implications: "It was my fault," "I should have done something different," "The world is entirely unsafe," "I am permanently damaged." CPT involves both cognitive restructuring techniques to challenge these beliefs and, in most protocols, a written account of the trauma that facilitates emotional processing.
CPT has a comparable evidence base to PE, with multiple RCTs finding large effect sizes across diverse populations.
A key practical advantage of CPT is that it is somewhat more flexible in delivery - it can be delivered in group format and via telehealth with good effectiveness, making it more accessible in settings where intensive individual therapy is not available.
EMDR
Eye Movement Desensitization and Reprocessing (EMDR), developed by Francine Shapiro, has comparable outcome data to PE and CPT and is classified as an evidence-based treatment by major clinical bodies. Its mechanism remains controversial.
The active ingredient of bilateral eye movements has been questioned by component studies; some find that the eye movements add benefit while others find no difference between EMDR with and without the bilateral stimulation.
Many researchers believe that EMDR's effectiveness derives from its exposure component. The controversy about mechanism does not diminish its clinical utility.
MDMA-Assisted Therapy
The most significant recent development in PTSD treatment is the Phase 3 clinical trial program for MDMA-assisted psychotherapy, conducted by the Multidisciplinary Association for Psychedelic Studies (MAPS).
MDMA (3,4-methylenedioxymethamphetamine) is a monoamine-releasing agent that elevates serotonin, dopamine, and norepinephrine while also reducing amygdala reactivity to threat stimuli and increasing oxytocin and prolactin release - a pharmacological profile that appears to facilitate the processing of traumatic memories by reducing the fear response while maintaining the ability to engage cognitively with the content.
In Phase 3 trials published in Nature Medicine in 2021, 67% of participants receiving MDMA-assisted therapy no longer met PTSD diagnostic criteria at follow-up, compared to 32% in the placebo with therapy group - an effect size substantially larger than existing pharmacological treatments and comparable to best psychological treatments.
The therapy consists of two to three eight-hour MDMA sessions embedded within a longer therapeutic relationship.
The FDA was expected to review the treatment, but as of 2024 had declined approval due to questions about blinding methodology and site-related issues in the trial data, while acknowledging the clinical significance of the efficacy findings. Research continues.
Reconsolidation and Propranolol
An alternative pharmacological approach targets memory reconsolidation - the window after a memory is reactivated during which it becomes labile and can be modified before being re-stored.
The beta-blocker propranolol, which blocks noradrenergic activity, has been found in several studies to reduce conditioned fear responses when administered after memory reactivation, potentially by disrupting the reconsolidation of the fear memory.
Results have been mixed in clinical PTSD populations, and the approach has not yet demonstrated clinical effectiveness comparable to the established psychotherapies.
Complex PTSD and Developmental Trauma
Judith Herman's 1992 book "Trauma and Recovery" argued that the existing PTSD diagnosis, developed primarily from the experience of combat veterans and disaster survivors, failed to capture the specific sequelae of prolonged, repeated interpersonal trauma - particularly childhood abuse, domestic captivity, and torture.
Herman proposed that chronic trauma produced a syndrome she called "complex PTSD" or "disorders of extreme stress not otherwise specified" (DESNOS), characterized by severe disturbances in affect regulation, consciousness and self-perception, and interpersonal relationships, in addition to the standard PTSD symptoms.
The ICD-11, published by the World Health Organization and effective from 2022, formally recognized Complex PTSD (C-PTSD) as a distinct diagnosis alongside standard PTSD. The DSM-5 did not include C-PTSD as a separate category, though it added a dissociative subtype of PTSD and other specifiers that partially address the clinical picture.
C-PTSD is associated with childhood abuse and neglect, domestic violence, political imprisonment, and other forms of prolonged captivity or victimization.
Its clinical presentation is characterized by persistent emotional dysregulation - explosive rage alternating with emotional numbing, chronic depression, and self-destructive behavior - along with severe disturbances in self-perception (pervasive shame, guilt, and sense of being permanently damaged) and difficulty forming and sustaining relationships.
Standard trauma-focused treatments like PE and CPT were developed and validated for single-incident adult trauma, and there is debate about whether they require modification for C-PTSD.
Many clinicians recommend a phase-based approach beginning with stabilization - emotion regulation skills and trauma-focused relationship building - before moving to direct trauma processing.
Moral Injury: A Distinct Wound
Jonathan Shay, a psychiatrist who worked for decades with Vietnam veterans at the Boston Veterans Outreach Center, argued in his 1994 book "Achilles in Vietnam" that much of what combat veterans experience is better captured by the concept of moral injury than by the PTSD diagnosis.
Moral injury, as Shay and later researchers have defined it, refers to harm to a person's moral foundations from perpetrating, witnessing, or failing to prevent actions that violate deeply held moral beliefs, particularly when the transgression occurs within a context of betrayal by legitimate authority.
Shay drew on Homer's "Iliad" to illuminate the experience of soldiers who were commanded to do things they knew to be wrong, who witnessed atrocities committed by allies, and who returned to a society that did not want to hear about what they had done and seen.
The injury, he argued, was not primarily a fear-based response (the core of PTSD) but a wound to moral identity and the sense of justice that constitutes the self.
Moral injury and PTSD frequently co-occur but are conceptually and clinically distinct. Moral injury responds poorly to fear-based treatments like prolonged exposure; it may require approaches focused on forgiveness, meaning-making, and social recognition rather than on fear extinction.
The concept has gained traction in military mental health and has been applied to other professional groups - healthcare workers who were unable to provide adequate care during the COVID pandemic, for instance, or soldiers who follow orders they believe to be unethical.
Related Articles
For an exploration of the broader psychological concept of trauma, see What Is Trauma?. For the physiological mechanisms of stress on the body, see How Stress Damages the Body. For the psychological process of losing someone, see How Grief Works.
Sources & Further Reading
- Bremner, J. D., Randall, P., Scott, T. M., Bronen, R. A., Seibyl, J. P., Southwick, S. M., Delaney, R. C., McCarthy, G., Charney, D. S., & Innis, R. B. (1995). MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. American Journal of Psychiatry, 152(7), 973-981. DOI: 10.1176/ajp.152.7.973
- Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. Oxford University Press.
- Gilbertson, M. W., Shenton, M. E., Ciszewski, A., Kasai, K., Lasko, N. B., Orr, S. P., & Pitman, R. K. (2002). Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neuroscience, 5(11), 1242-1247. DOI: 10.1038/nn958
- Herman, J. L. (1992). Trauma and Recovery: The Aftermath of Violence - From Domestic Abuse to Political Terror. Basic Books.
- Kardiner, A. (1941). The Traumatic Neuroses of War. Paul B. Hoeber.
- Mitchell, J. M., Bogenschutz, M., Lilienstein, A., Harrison, C., Kleiman, S., Parker-Guilbert, K., Ot'alora G., M., Garas, W., Paleos, C., Gorman, I., Nicholas, C., Mithoefer, M., Carlin, S., Poulter, B., Mithoefer, A., Quevedo, S., Gregory, R., Hoover, D., Zubaran, C.... & Doblin, R. (2021). MDMA-assisted therapy for severe PTSD: A randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine, 27(6), 1025-1033. DOI: 10.1038/s41591-021-01336-3
- Resick, P. A., Monson, C. M., & Chard, K. M. (2016). Cognitive Processing Therapy for PTSD: A Comprehensive Manual. Guilford Press.
- Shay, J. (1994). Achilles in Vietnam: Combat Trauma and the Undoing of Character. Simon and Schuster.
- Shapiro, F. (1989). Eye movement desensitization: A new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry, 20(3), 211-217. DOI: 10.1016/0005-7916(89)90025-6
- Yehuda, R., Southwick, S. M., Krystal, J. H., Bremner, D., Charney, D. S., & Mason, J. W. (1993). Enhanced suppression of cortisol following dexamethasone administration in posttraumatic stress disorder. American Journal of Psychiatry, 150(1), 83-86. DOI: 10.1176/ajp.150.1.83
Health note: This article is general educational information about how a topic works, not medical, psychological, or mental-health advice, diagnosis, or treatment. Everyone's situation is different, and research findings describe groups, not individuals.
If you are struggling or have concerns about your health, please talk to a qualified professional such as a doctor or licensed therapist.
If you are in crisis or thinking about harming yourself, contact your local emergency services or a crisis line right away, in the US you can call or text 988 (Suicide & Crisis Lifeline); elsewhere, find local lines at findahelpline.com.
Frequently Asked Questions
What is PTSD and how is it different from normal stress reactions?
Post-traumatic stress disorder (PTSD) is a psychiatric condition that can develop following exposure to a traumatic event, one involving actual or threatened death, serious injury, or sexual violence. DSM-5 defines PTSD through four symptom clusters: intrusion (unwanted intrusive memories, flashbacks, nightmares, intense psychological distress when exposed to reminders); avoidance (avoiding distressing memories, thoughts, feelings, or external reminders of the trauma); negative alterations in cognitions and mood (persistent negative beliefs about oneself or the world, distorted blame, persistent negative emotions, diminished interest in activities, feeling detached from others, inability to experience positive emotions); and alterations in arousal and reactivity (hypervigilance, exaggerated startle response, sleep disturbance, irritability, reckless behavior, problems with concentration).The distinction between PTSD and normal acute stress responses is principally one of persistence and severity. Acute stress reactions following trauma are nearly universal, most people exposed to a serious traumatic event will experience some intrusive thoughts, hyperarousal, and sleep disturbance in the days and weeks following the event. These acute responses are adaptive in the short term: they maintain alertness to potential ongoing threat and facilitate emotional processing of the event. For most people, these responses diminish over weeks to months as the trauma is integrated.PTSD is diagnosed when this resolution does not occur, when symptoms persist for more than one month following the trauma, cause significant distress or functional impairment, and are not attributable to substance use or another medical condition. Approximately 70% of people who experience a potentially traumatic event do not develop PTSD, suggesting that resilience, not trauma response, is the modal outcome. Risk factors for persistent PTSD include prior trauma history, the severity and duration of the traumatic event, peritraumatic dissociation (feeling detached from oneself during the event), lack of social support afterward, and pre-existing anxiety or depression.
What happens in the brain during PTSD?
PTSD is best understood neuroscientifically as a disorder of fear memory, specifically, a failure of normal fear extinction and contextual gating processes that prevent traumatic fear memories from being appropriately modulated over time.In normal fear conditioning, a neutral stimulus (a sound, a smell, a visual cue) that is paired with a threatening unconditioned stimulus (a violent event) acquires the capacity to trigger a fear response, the conditioned stimulus becomes a conditioned fear cue. This process depends critically on the amygdala, a subcortical structure that processes threat signals and generates autonomic and behavioral fear responses. The hippocampus normally provides contextual information, this cue was paired with danger in that specific context, not in all contexts, allowing the prefrontal cortex to inhibit amygdala fear responses when the context signals safety. In PTSD, this prefrontal regulatory control appears to be impaired: fear responses are triggered by cues that resemble the original trauma regardless of current safety context.Several neurobiological findings characterize PTSD. Rachel Yehuda’s research at the Bronx Veterans Affairs Medical Center documented a paradoxical pattern: while normal stress responses involve elevated cortisol (the primary glucocorticoid stress hormone), PTSD patients showed lower cortisol levels and an enhanced suppression of cortisol by dexamethasone, suggesting a hypersensitive HPA axis negative feedback loop. This finding, replicated in multiple populations, suggested that PTSD involves dysregulation of stress hormone systems rather than simply an excess stress response.Structural neuroimaging studies have consistently found smaller hippocampal volumes in individuals with PTSD compared to trauma-exposed controls without PTSD and to healthy non-exposed controls. The Bremner group at Yale was among the first to report this, finding approximately 8% smaller hippocampal volume in Vietnam veterans with PTSD. A key unresolved question is whether reduced hippocampal volume is a consequence of trauma and PTSD, or a pre-existing vulnerability that predisposes individuals to developing PTSD after trauma.
Who is most at risk for PTSD?
PTSD does not develop in everyone who experiences a traumatic event, lifetime prevalence in the United States is approximately 7-8% of the general population, meaning that most people who experience potentially traumatic events do not develop the condition. However, PTSD risk varies substantially based on the type of trauma, individual characteristics, and contextual factors.Trauma type is one of the strongest predictors of PTSD risk. The highest conditional risk, the probability of developing PTSD given exposure to a particular type of trauma, is associated with sexual assault (approximately 45-65%), combat exposure (20-30% in deployed veterans from recent conflicts), and childhood abuse. Tragedies such as accidents, natural disasters, and witnessing violence carry lower but still elevated risk. The severity, duration, proximity to the threat, and the degree to which the event involves human perpetration (assault, sexual violence, torture) all increase risk relative to accidents and natural disasters.Sex is a robust risk factor: women develop PTSD at approximately twice the rate of men after controlling for trauma type exposure, a finding that persists across cultures. The mechanisms are debated, possible contributors include differences in trauma type (women are more likely to experience sexual assault), differences in cortisol reactivity, neurobiological differences in fear extinction, and social factors affecting help-seeking and disclosure.Psychological risk factors include prior trauma history (particularly childhood trauma), pre-existing anxiety, depression, or other psychiatric conditions, and peritraumatic dissociation, a feeling of unreality, depersonalization, or emotional detachment during the traumatic event that is among the strongest prospective predictors of PTSD development. Protective factors include strong social support, access to early psychosocial intervention, active coping styles, and the absence of prior psychiatric history.
What treatments have the strongest evidence?
PTSD treatment research has advanced substantially since the condition was first formally recognized in 1980, and several treatments now have strong randomized controlled trial evidence. The psychological treatments with the most robust evidence bases are Prolonged Exposure therapy and Cognitive Processing Therapy.Prolonged Exposure (PE), developed by Edna Foa and her colleagues at the University of Pennsylvania and now at the Center for the Treatment and Study of Anxiety, is based on emotional processing theory and involves two main components: imaginal exposure (repeated, prolonged revisiting of the traumatic memory in imagination, with detailed recounting) and in vivo exposure (graduated confrontation with avoided trauma-related situations, people, and objects in daily life). Meta-analyses of PE consistently find large effect sizes, and it has been designated a gold-standard treatment by the Department of Veterans Affairs.Cognitive Processing Therapy (CPT), developed by Patricia Resick and colleagues, targets the cognitive distortions, ‘stuck points’, that maintain PTSD by preventing the natural processing of the traumatic event. It includes both cognitive restructuring of distorted beliefs and, in some versions, written accounts of the traumatic experience. Like PE, CPT has strong evidence from multiple RCTs across diverse trauma populations.EMDR (Eye Movement Desensitization and Reprocessing) is discussed separately. Among pharmacological treatments, the SSRIs sertraline and paroxetine are FDA-approved for PTSD, with modest effect sizes. The most exciting recent development is MDMA-assisted therapy, which is discussed in a separate question.A 2020 Cochrane review examining pharmacological treatments for PTSD found that while SSRIs produced statistically significant improvements, their effect sizes were small to moderate and clinical significance was limited for many patients, underscoring the importance of trauma-focused psychological therapies as first-line treatments.
What is EMDR and does it work?
Eye Movement Desensitization and Reprocessing (EMDR) was developed by clinical psychologist Francine Shapiro following a serendipitous observation in 1987: she noticed that making rapid lateral eye movements while thinking about distressing memories appeared to reduce their emotional charge. She developed this observation into a structured psychotherapy protocol involving eight phases, during which patients focus on traumatic memories while simultaneously engaging in bilateral sensory stimulation, typically a therapist-guided finger movement tracking task that elicits rapid lateral eye movements, though alternatives include auditory tones or tactile taps.The evidence for EMDR’s effectiveness is robust. Multiple randomized controlled trials and meta-analyses have found that EMDR significantly reduces PTSD symptoms, with effect sizes comparable to Prolonged Exposure and Cognitive Processing Therapy. It is designated as an evidence-based treatment by the World Health Organization, the VA/DoD Clinical Practice Guidelines, and the American Psychological Association.What has been more controversial is the mechanism. The eye movement component was Shapiro’s theorized ‘active ingredient,’ and she proposed that bilateral stimulation facilitated the reprocessing of traumatic memories through a mechanism involving working memory and the orienting response. However, component analyses, studies comparing full EMDR to versions without the eye movement component, have produced mixed results, with some showing that the eye movements add benefit and others showing no difference. Some researchers argue that the therapeutic effectiveness of EMDR derives from the exposure component (attending to the traumatic memory) rather than the eye movements, making it a form of imaginal exposure with an unusual procedural protocol.This mechanistic uncertainty does not diminish its clinical value, a treatment can work without our understanding exactly how. But it raises questions about the theoretical framework Shapiro developed, and the debate about mechanism has made EMDR more controversial among researchers than its outcome data would suggest it should be.
What is complex PTSD?
Complex PTSD (C-PTSD) refers to a pattern of symptoms that emerges specifically from prolonged, repeated trauma, particularly when the trauma occurs in contexts from which escape is difficult or impossible, such as childhood abuse, domestic violence, prolonged captivity, or torture. The concept was introduced by psychiatrist Judith Herman in her landmark 1992 book ‘Trauma and Recovery,’ in which she argued that the existing PTSD diagnosis, developed primarily based on the experience of combat veterans and disaster survivors, failed to capture the full range of sequelae from chronic interpersonal trauma.Herman proposed that repeated, inescapable trauma produces a recognizable syndrome extending beyond standard PTSD symptoms to include three additional feature clusters: severe disturbances in affect regulation (difficulty modulating emotions, frequent explosive anger or complete emotional numbing, chronic feelings of emptiness and hopelessness); disturbances in consciousness and self-perception (amnesia, dissociation, persistent shame, self-blame, and a fundamentally altered sense of identity); and disturbances in relations with others (difficulty trusting, revictimization patterns, inability to maintain relationships).After years of debate about whether complex PTSD was a distinct diagnosis or a severe form of standard PTSD, the 11th revision of the International Classification of Diseases (ICD-11), published by the World Health Organization in 2018 and effective from 2022, formally included C-PTSD as a distinct diagnosis alongside PTSD. The DSM-5 did not include C-PTSD, instead incorporating a ‘PTSD with prominent dissociative features’ specifier and a separate ‘Reactive Attachment Disorder’ for children, a difference in classification that reflects ongoing scientific disagreement about the nature of the condition.The clinical implications are significant: standard trauma-focused treatments like Prolonged Exposure and CPT were developed for single-incident trauma and may need to be preceded by stabilization phases for individuals with complex PTSD whose emotion regulation is severely impaired.