Empathy is one of the most frequently invoked virtues in contemporary life. Leaders are told to lead with it. Employers list it in job descriptions. Therapists train in it. Politicians perform it.
And yet, despite its ubiquity, empathy is poorly understood, frequently conflated with related concepts, and the subject of genuine scientific and philosophical dispute about whether it is even the virtue it is made out to be.
This article is a clear-eyed examination of what empathy actually is, what the science says about its mechanisms and limits, and why one prominent psychologist has built a credible case that too much of the wrong kind of empathy may make us worse at helping people, not better.
Defining the Concept: Empathy Is Not One Thing
The word "empathy" was coined in English by the psychologist Edward Titchener in 1909 as a translation of the German Einfühlung ("feeling into"), a concept originally developed in aesthetics to describe the experience of projecting oneself imaginatively into a work of art.
By the mid-20th century it had been applied to interpersonal psychology, and by the 21st century it had become shorthand for almost any form of social sensitivity.
This breadth of usage has created real confusion, because what researchers mean by empathy encompasses at least three distinct psychological processes that can operate independently and even conflict with each other.
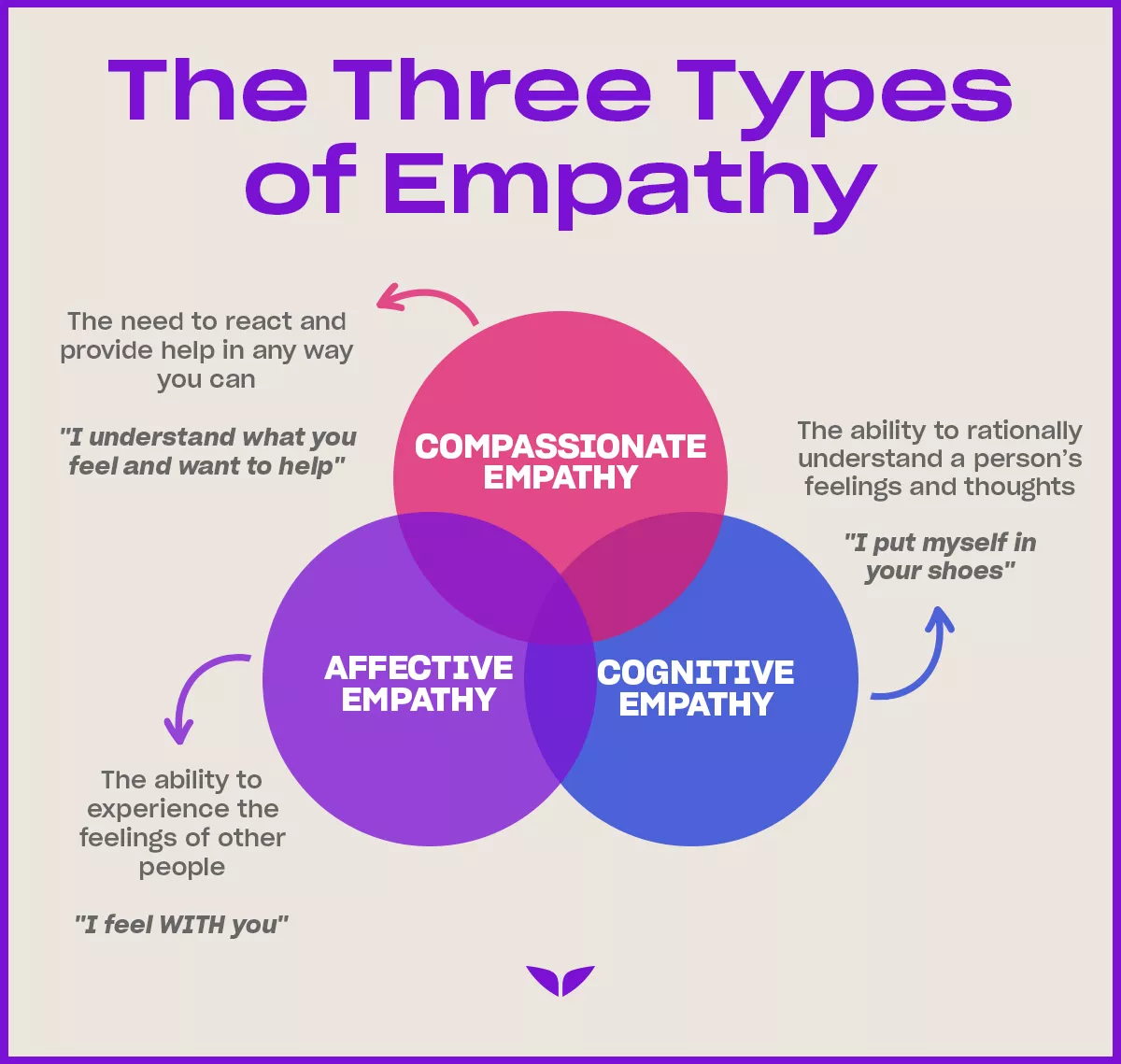
Affective Empathy
Affective empathy is the automatic, often involuntary experience of sharing or resonating with another person's emotional state.
When you wince watching someone stub their toe, feel a knot of dread when a friend describes a difficult conversation, or find yourself laughing before a joke is finished because the person telling it is already laughing - these are instances of affective empathy.
The response happens quickly, often before conscious awareness, and it involves something like an echo of the other person's emotional state in your own body and mind.
This form of empathy is largely automatic. It is the basis of what psychologists call emotional contagion - the tendency for moods and emotions to spread between people through mimicry, facial feedback, and synchronized physiological states.
Newborns cry when they hear other babies cry. Laughter is contagious in crowds. Sadness in a room full of grieving people has a way of landing.
Cognitive Empathy
Cognitive empathy - also called theory of mind or mentalizing - is the ability to accurately represent and understand another person's mental states: their beliefs, intentions, desires, knowledge, and emotional condition. It does not require feeling what the other person feels. It requires modeling what they feel.
A skilled negotiator exercises cognitive empathy when mapping an opponent's interests and likely responses. A novelist exercises it when writing convincingly from a character's point of view. A psychologist exercises it during case formulation, when building a model of what it is like to be the patient in front of them.
Cognitive and affective empathy are doubly dissociable - they can come apart in both directions.
Research on autism spectrum conditions has found that many autistic individuals have intact or even heightened affective empathy (they genuinely feel others' distress, sometimes to an overwhelming degree) but face specific challenges with theory of mind tasks, particularly when interpreting ambiguous social cues.
The earlier framing of autism as a disorder of empathy was imprecise; it more accurately involves specific challenges in cognitive mentalizing rather than an absence of emotional resonance.
Conversely, individuals high in psychopathic traits may retain strong cognitive empathy - they can model others' mental states accurately, including predicting what will hurt them - while showing reduced affective resonance with others' suffering.
Compassionate Empathy
Compassionate empathy (sometimes simply called compassion) involves feeling warm concern for another's suffering and being motivated to help, without necessarily absorbing or mirroring the suffering itself.
It is the form most closely aligned with what most people intuitively want from an empathic other: someone who cares about what you are going through and wants to help, but who has not become so overwhelmed by your distress that they are no longer functional.
Tania Singer and Olga Klimecki at the Max Planck Institute have documented the neural distinction between empathic resonance and compassion using neuroimaging.
Their work found that compassion training - through loving-kindness meditation - activates circuits associated with positive affect, affiliation, and reward (including medial orbitofrontal cortex and striatum), whereas empathic pain resonance activates distress-related circuits in the anterior insula and anterior cingulate cortex.
| Type | Core process | Voluntary? | Neural signature |
|---|---|---|---|
| Affective empathy | Emotional resonance/sharing | Mostly automatic | Anterior insula, anterior cingulate cortex |
| Cognitive empathy | Mental state modeling | Largely deliberate | Medial prefrontal cortex, temporoparietal junction |
| Compassionate empathy | Warm concern + motivation to help | Deliberate and cultivated | Medial OFC, striatum, posterior insula |
The Science of Pain Empathy
Pain empathy is one of the most studied forms in neuroscience because pain is reliably inducible and quantifiable.
Claus Lamm, Jean Decety, and Tania Singer's 2011 meta-analysis synthesized 116 neuroimaging studies involving 2,564 participants and found that observing another person in pain consistently activates the anterior insula and the anterior and mid cingulate cortex.
These are not motor areas. They are areas involved in interoception - the monitoring of internal body states - and in the affective, motivational dimensions of pain.
The implication is that witnessing pain activates something closer to "this matters and something is wrong" than "I am experiencing the same sensory experience as the person in pain."
This distinction is important. Empathy for pain does not mean you experience the other person's pain. It means you register its significance.
Singer's research also showed that empathic pain responses are profoundly context-dependent. Prior cooperation with the person in pain increased empathic neural response.
Prior unfair treatment by that person reduced it - particularly in men, who showed more neural activity in reward regions (consistent with Schadenfreude) when an unfair player experienced pain.
The empathic response is not an impartial reading of another person's state; it is filtered through social context, relationship history, and current motivation.
"Empathy is a spotlight, not a floodlight. It illuminates specific people in specific moments based on who we are already oriented toward." - adapted from Paul Bloom, Against Empathy (2016)
The Dark Triad and Empathy Deficits
The dark triad refers to a cluster of three personality traits that share a common core of callousness and social manipulation: narcissism, Machiavellianism, and psychopathy. These traits correlate negatively with affective empathy but show a more complex relationship with cognitive empathy.
Narcissism involves grandiosity, entitlement, and a need for admiration. Narcissists tend to show reduced empathic concern for others but often retain and deploy cognitive perspective-taking, particularly in contexts where understanding others' vulnerabilities serves their own goals.
Machiavellianism involves strategic, detached manipulation of others for personal benefit. High Machiavellians tend to explicitly suppress emotional responses and rely on cold cognitive modeling to navigate social situations.
Psychopathy has received the most research attention in relation to empathy. Robert Hare's Psychopathy Checklist Revised (PCL-R) includes factors relating to callousness, shallow affect, lack of remorse, and failure to be deterred by others' distress - all suggesting affective empathy deficits.
Research by Jean Decety and colleagues found that individuals with high PCL-R scores show reduced automatic neural responses to others' pain but can show more normal responses when explicitly instructed to imagine what the person is feeling.
This finding suggests the deficit is in automatic, involuntary empathic engagement rather than capacity per se - a distinction with significant clinical and behavioral implications.
| Trait | Affective empathy | Cognitive empathy | Key behavioral consequence |
|---|---|---|---|
| Narcissism | Reduced | Often intact | Uses perspective-taking for advantage, not care |
| Machiavellianism | Suppressed | High | Coldly strategic social manipulation |
| Psychopathy | Impaired automatically | Can activate deliberately | Reduces guilt and restraint from causing harm |
Paul Bloom's Argument Against Empathy
Paul Bloom, a psychology professor at Yale and later the University of Toronto, published Against Empathy: The Case for Rational Compassion in 2016. The book's thesis is deliberately provocative but grounded in a genuine empirical argument.
Bloom's core claim is that affective empathy is a biased, unreliable, and easily manipulated guide to moral action, and that it produces worse outcomes than impartial, evidence-based compassion.
The Identifiable Victim Effect
Psychologists have long documented the identifiable victim effect: a single identified individual with a name and a face generates far more charitable giving, policy support, and emotional mobilization than statistical descriptions of larger numbers of people in equal or greater need.
A photo of a child with a name and a story will generate more donation than the statistic that thousands of children died from preventable disease today.
This is not a flaw in the statistical framing. It is a feature of how affective empathy works. Empathy is activated by salience, proximity, and identifiability. It is not activated by scale. We cannot empathize with a million people; we can only empathize with a person.
The result is that emotionally compelling individual stories drive resource allocation in ways that bear no relationship to aggregate need.
Empathy as a Political Weapon
Bloom argues that empathy is routinely weaponized by political actors precisely because it bypasses rational evaluation.
By choosing which face represents a cause, which story gets told, which victim gets named, propagandists and politicians can generate empathic responses that support policies those same audiences might reject if presented with aggregate data.
The deliberate selection of sympathetic individuals to represent complex policy positions is a manipulation of empathy, not an argument.
Empathy Is Biased Toward the Similar
Research consistently shows that empathy is stronger for individuals who resemble us - in appearance, background, or group membership. In-group members' pain activates greater empathic neural responses than out-group members' pain.
This means empathy, left to operate without correction, reinforces existing group loyalties rather than expanding moral concern.
The Case for Rational Compassion
Bloom's alternative is not coldness or indifference. He advocates for rational compassion: a genuine concern for others' welfare that is guided by evidence about where help is most needed and most effective, rather than by which individuals generate the strongest emotional pull.
Effective altruism - the movement that tries to maximize the good done by charitable giving through rigorous evaluation of impact - is one institutional expression of this orientation.
Empathy Fatigue: The Cost of Absorbing Others' Suffering
Empathy fatigue (frequently called compassion fatigue, though the distinction between the two concepts has clinical significance) is the emotional and physical exhaustion that results from chronic exposure to others' suffering, particularly when that exposure involves absorbing or resonating with the suffering rather than maintaining compassionate concern from a stable base.
The condition was first systematically described in the context of nursing by Joinson (1992) and later elaborated by Charles Figley, whose work on secondary traumatic stress in therapists and counselors documented that caregiving professionals can develop trauma-like symptoms not from direct traumatic events but from sustained exposure to clients' trauma narratives.
Who Is Most Affected
Healthcare workers, therapists, social workers, emergency responders, and humanitarian aid workers are at highest risk.
Research suggests that the risk is highest when empathic engagement is high and personal resources are low - when work demands are intense, boundaries between professional and personal life are blurred, and self-care practices are absent.
Singer and Klimecki's neuroscience research provided a mechanistic account: empathic resonance with others' pain activates distress circuits and produces negative affect. Over time and without recovery, this is not sustainable.
Compassion training that shifts orientation from resonance to warm concern activates different, less distressing circuits and shows greater long-term resilience.
Practical Implications
For individuals in caregiving roles, the research suggests:
- Boundary maintenance is not callousness; it is a prerequisite for sustainable care.
- Supervision and processing of vicarious trauma reduces accumulation.
- Shifting from empathic resonance to compassionate concern - feeling for rather than feeling with - is a trainable skill with measurable neural and psychological benefits.
- Self-compassion practices buffer against depletion and are associated with lower burnout rates in healthcare settings.
Empathy in the Workplace
The organizational literature on empathy has expanded substantially since the late 2010s, partly in response to research linking leader empathy to team performance, psychological safety, and employee retention.
What the Research Shows
A 2021 study published in Harvard Business Review based on surveys of thousands of employees found that empathy from direct managers was the single strongest predictor of innovation, engagement, and intention to stay. Korn Ferry research has consistently ranked empathy among the top competencies distinguishing high-performing leaders.
However, workplace empathy research often conflates affective and cognitive empathy, and conflates empathy with active listening, feedback quality, and interpersonal attentiveness.
The more precise finding may be that cognitive empathy - accurately modeling what teammates and direct reports are experiencing and needing - is what drives performance outcomes, rather than emotional resonance per se.
Limits of Empathy in Organizational Settings
There are documented costs. Research has found that:
- Managers who engage in excessive affective empathy with subordinates' distress show higher burnout and are sometimes less effective at delivering critical feedback.
- Empathic concern can interfere with impartial decision-making when personal empathic connections distort evaluation.
- In-group favoritism in performance evaluations is partly an empathy-mediated effect: we model the inner lives of people we feel close to more richly than those we feel distant from, and rate them more favorably.
Practical Empathy at Work: What Actually Helps
| Practice | What it targets | Evidence base |
|---|---|---|
| Perspective-taking instructions | Cognitive empathy | Moderate-strong in experimental settings |
| Active listening training | Accuracy of empathic understanding | Moderate |
| Psychological safety norms | Creates conditions for genuine sharing | Strong (Edmondson, 1999) |
| Compassion training programs | Reduces burnout in care roles | Moderate (Singer & Klimecki, 2014) |
| Reducing time pressure | Allows empathic processing | Experimental evidence (Darley & Batson) |
Empathy vs. Sympathy: Why the Distinction Matters
These terms are used interchangeably in everyday speech but describe meaningfully different orientations.
Sympathy is feeling concern or sorrow for another's situation from your own emotional position. You recognize that someone is suffering and you feel something about it, but you remain situated in your own experience. You feel for them.
Empathy (in the affective sense) involves feeling with them - entering their emotional experience, at least partially, and resonating with their state rather than merely observing it from outside.
The distinction is not merely semantic. In clinical and caregiving contexts, sympathy may be less effective at communicating understanding than empathy, because the person experiencing difficulty may sense whether the other person has genuinely tried to understand their internal experience or is merely feeling sorry for them.
Researcher Brene Brown's widely shared distinction - sympathy drives disconnection, empathy drives connection - captures this asymmetry, though her framing has been criticized for being too binary.
The more nuanced picture is that different situations call for different responses. Someone in acute distress may need the felt sense that another person is truly with them (affective empathy). Someone navigating a complex decision may need accurate perspective-taking without emotional flooding (cognitive empathy).
Someone dealing with a prolonged difficult situation may need sustained warm concern and practical support (compassionate empathy) more than emotional resonance that is not maintainable.
What the Evidence Actually Supports
After decades of research, several findings are robust:
- Empathy is not a single thing. Affective and cognitive empathy are separable, supported by partially distinct neural systems, and can dissociate in both clinical and subclinical populations.
- Empathic accuracy is surprisingly low. Studies of how well people actually read others' emotional states (as opposed to believing they do) consistently find that accuracy is modest and does not improve substantially with training alone.
- Compassionate concern is more sustainable than empathic absorption. Singer and Klimecki's work provides the clearest evidence that care without taking on others' distress is both possible and neurologically distinct from empathic resonance.
- Empathy is biased. It favors the visible, the proximate, the similar, and the identifiable. Without deliberate correction, these biases operate automatically.
- The virtues of empathy are real but limited. Empathy promotes prosocial behavior and reduces dehumanization. It is not sufficient for good moral reasoning and can actively mislead it when bias and scale problems are not corrected.
The research suggests that the goal is not maximum empathy but the right kind of empathic engagement for the situation: cognitive accuracy when understanding is needed, compassionate concern when sustaining care over time, and the willingness to override empathic pull with impartial reasoning when scale and equity demand it.
Frequently Asked Questions
What are the three types of empathy?
Psychologists identify three main types: affective empathy (feeling what another person feels, an involuntary emotional resonance), cognitive empathy (understanding what another person is experiencing without necessarily sharing the feeling), and compassionate empathy (feeling concern for someone’s suffering and being moved to help). These three can operate independently. A skilled surgeon may have high cognitive empathy and deliberately muted affective empathy to perform calmly under emotional pressure.
What is empathy fatigue and who is most at risk?
Empathy fatigue, also called compassion fatigue, is the emotional and physical exhaustion that results from chronic exposure to others’ suffering, particularly when one absorbs that suffering rather than maintaining compassionate concern from a stable emotional base. Healthcare workers, therapists, emergency responders, and social workers are most at risk. Research by Tania Singer and Olga Klimecki found that pure empathic resonance with pain activates distress circuits and is not sustainable over time, whereas compassion training activates reward and affiliation circuits and shows greater resilience.
What is Paul Bloom's argument against empathy?
In his 2016 book Against Empathy, psychologist Paul Bloom argues that affective empathy is a poor guide to moral action because it is biased toward individuals who are visible, proximate, and similar to us. We empathize easily with an identifiable individual in front of us but poorly with statistical victims of distant policy failures. This bias can be exploited by politicians and propagandists, and it leads to resource allocation that reflects emotional salience rather than actual need. Bloom advocates for rational compassion instead: impartial concern for suffering based on evidence rather than empathic pull.
Do people with dark triad traits lack empathy?
People high in dark triad traits (narcissism, Machiavellianism, and psychopathy) tend to show reduced affective empathy, meaning they do not automatically resonate with others’ distress. However, research suggests they often retain cognitive empathy and may even deploy it strategically to identify and exploit others’ vulnerabilities. Psychopathy in particular involves a specific deficit in automatic empathic engagement rather than a complete absence of empathic capacity, since individuals can sometimes engage empathically when explicitly motivated to do so.
How can empathy be developed in the workplace?
Workplace empathy can be developed through perspective-taking exercises, structured listening practices, and reducing cognitive load during interpersonal interactions (since empathy requires mental resources that stress depletes). Research suggests that perspective-taking instructions alone improve empathic accuracy in brief interactions. Longer-term, psychological safety in teams creates the conditions under which people share their genuine states, giving others more accurate signal to empathize with. Training in compassion rather than raw empathic absorption may be more sustainable for people in high-stress care or service roles.