The human body is not a single organism but an ecosystem. Trillions of microorganisms - bacteria, archaea, fungi, viruses, and protists - live in and on us, concentrated overwhelmingly in the colon.
Collectively, these organisms and their genomes constitute the human microbiome: a community whose aggregate metabolic activity, immune interactions, and neurological signaling influence human health in ways that scientific research is only beginning to characterize systematically.
The microbiome has become one of the most intensively studied areas in biomedical science. Publications on the gut microbiome increased from roughly 500 per year in 2005 to over 10,000 per year by 2020.
This explosion of research has produced genuine insights - particularly about the microbiome's role in immune development and the striking therapeutic success of fecal microbiome transplantation for recurrent Clostridioides difficile infection - alongside a great deal of premature enthusiasm, oversimplified popular science, and commercial products that outrun their evidence base by considerable distances.
Understanding the microbiome requires distinguishing carefully between what the science has established robustly, what is promising but preliminary, and what is marketing dressed in scientific language.
How Many Microorganisms Does the Human Body Host?
For decades, a widely repeated claim held that bacterial cells in the human body outnumber human cells by roughly ten to one - implying that we are "more microbe than human." The figure appeared in textbooks, popular science books, and countless articles.
It originated from a back-of-envelope estimate made by microbiologist Thomas Luckey in 1972 that was never rigorously derived but became canonical through repetition.
In 2016, Ron Sender, Shai Fuchs, and Ron Milo published a careful reassessment in Cell that revised the figure dramatically.
Using updated estimates of both bacterial and human cell counts - and recognizing that the original calculation had overestimated bacterial density in the colon and underestimated the number of human cells - they concluded that the ratio is approximately 1.3:1, not 10:1.
A 70-kilogram reference man contains roughly 38 trillion bacterial cells and approximately 30 trillion human cells. The margin of error in both estimates is large enough that the ratio could easily be near 1:1.
This matters for more than precision. The 10:1 figure was used rhetorically to suggest that our microbial passengers constitute a kind of second organism, a hidden self.
The corrected figure does not eliminate the microbiome's importance - 38 trillion bacteria with collective genomes encoding metabolic functions our own genome lacks are still enormously significant - but it reframes the relationship.
We are not "more microbe than human." The episode is instructive about how quantitative claims circulate in science communication: a single poorly documented estimate became accepted fact through repetition, citation from authority, and narrative appeal.
The Human Microbiome Project
The Human Microbiome Project (HMP) was a major NIH initiative launched in 2007 and running through 2016 in two phases, with a budget exceeding $170 million.
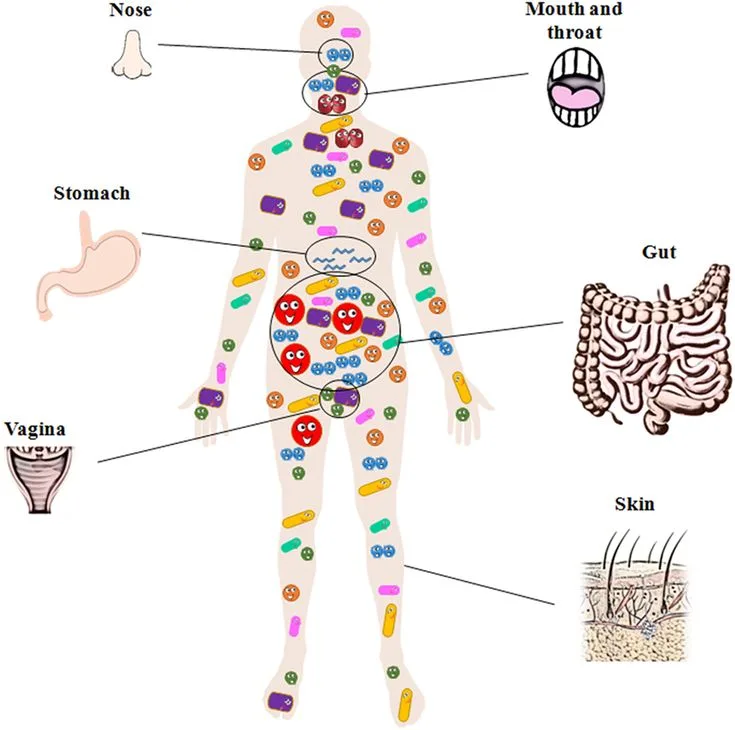
Its central goal was to characterize the normal microbial communities found at multiple body sites - gut, mouth, skin, vagina, nasal passages - in healthy adults, and to investigate how the microbiome relates to human health and disease.
The project faced a fundamental technical challenge: the vast majority of human-associated microorganisms cannot be cultured in the laboratory under standard conditions, meaning traditional bacteriology could only see a fraction of the community.
The HMP relied primarily on 16S ribosomal RNA gene sequencing, which targets a gene present in all bacteria but variable enough between species to serve as a molecular barcode.
By sequencing the 16S gene from all DNA in a sample - amplicon sequencing - researchers could identify which organisms were present without needing to culture them.
Shotgun metagenomics, sequencing all genetic material in a sample, added functional information: not just who is there but what metabolic capabilities they collectively encode.
Key findings from the HMP included:
The human microbiome is enormously variable between individuals - more variable than the human genome. Two healthy people may share only about 30% of their gut bacterial species.
Body sites differ dramatically in their microbial communities. The vaginal microbiome is typically dominated by a single Lactobacillus species and is far less diverse than the gut; high diversity in the vaginal microbiome is associated with bacterial vaginosis rather than being beneficial.
There is no single "healthy" gut microbiome composition. Early claims about universal beneficial ratios of bacterial phyla have not held up to scrutiny.
The microbiome is functionally redundant: different communities can perform similar metabolic functions even with different species compositions.
The HMP established the infrastructure and baseline data for the subsequent explosion of microbiome research, while also demonstrating that the field's early enthusiasm for simple correlations would need to give way to more sophisticated analysis of function, causation, and individual variation.
The Microbiome and the Immune System
The relationship between the gut microbiome and the immune system is one of the most important and best-documented aspects of microbiome science. The most compelling evidence comes from germ-free animal models: mice raised in sterile conditions with no microbial colonization have profoundly abnormal immune systems.
They have fewer and smaller lymph nodes and Peyer's patches (immune tissue in the gut), lower levels of secretory IgA antibodies, and abnormal T-cell populations.
Reintroducing specific bacteria partially or fully rescues these deficits, demonstrating that microbial signals during development are required for normal immune maturation.
Clostridia species in the colon - part of the normal human commensal community - induce the differentiation of regulatory T cells (Tregs), immune cells that suppress excessive inflammatory responses.
Studies by Sarkis Mazmanian's group and others showed that colonizing germ-free mice with a mixture of Clostridial strains restored normal Treg numbers and protected against experimental colitis and allergic responses.
The practical implication is that disruption of these communities - for instance by broad-spectrum antibiotics in early life - might impair the calibration of immune tolerance.
The "hygiene hypothesis," reformulated as the "old friends hypothesis" by Graham Rook, proposes that reduced exposure to the microorganisms with which humans co-evolved - through industrialized sanitation, small family size, and antibiotic use - has left the immune system inadequately calibrated against inappropriate inflammatory responses, contributing to rising rates of allergies, asthma, and autoimmune conditions.
Epidemiological patterns support this framework. Inflammatory bowel diseases (Crohn's disease and ulcerative colitis) are characterized by altered microbiome composition, though establishing whether dysbiosis (disturbed microbial community) causes IBD or results from it is methodologically challenging.
Children raised on farms with early exposure to diverse microbial environments have substantially lower rates of allergic disease than urban children - a pattern observed across multiple European cohort studies.
| Body Site | Dominant Organisms | Diversity | Health Association |
|---|---|---|---|
| Colon | Bacteroidetes, Firmicutes, Proteobacteria | Very high | High diversity generally favorable |
| Oral cavity | Streptococcus, Actinomyces, Prevotella | High | Dysbiosis linked to caries, periodontitis |
| Skin | Staphylococcus, Cutibacterium | Moderate | Dysbiosis linked to atopic dermatitis |
| Vagina | Lactobacillus (dominant) | Low (healthy) | High diversity linked to BV |
| Nasal passages | Staphylococcus, Corynebacterium | Low-moderate | Colonization affects respiratory health |
The Gut-Brain Axis
The gut-brain axis refers to the bidirectional communication network linking the central nervous system with the enteric nervous system (the extensive network of neurons embedded in the gut wall) and the gut microbiome.
Communication runs through multiple channels: the vagus nerve, which carries signals between gut and brain stem; immune mediators including cytokines; the hypothalamic-pituitary-adrenal (HPA) axis regulating the stress response; and a range of metabolites produced by gut bacteria.
Roughly 90-95% of the body's serotonin is produced in the gut, not the brain, and several gut bacteria influence serotonin synthesis.
Gut bacteria also produce gamma-aminobutyric acid (GABA), produce short-chain fatty acids that influence brain function, and can metabolize tryptophan through the kynurenine pathway relevant to mood regulation.
Animal experiments have been striking. Transferring gut microbiota from anxious mouse strains into germ-free recipients produced anxiety-like behaviors; the reverse transfer also worked in some studies.
John Cryan and Ted Dinan coined the term "psychobiotics" in 2013 to describe bacteria with potential mental health benefits, a concept that generated substantial popular and scientific attention.
However, the field has significant problems with overclaiming. Human trials of probiotics for depression and anxiety have produced mixed results; most have been small, short-term, and methodologically limited. The most rigorous systematic reviews find modest effects at best.
The mechanisms demonstrated in germ-free mouse models do not translate simply to humans with lifelong established microbiomes. The human gut-brain axis exists and is physiologically real, but confident claims that specific probiotic strains treat depression are currently well ahead of the evidence.
The Microbiome and Obesity
The relationship between the gut microbiome and obesity is one of the most intriguing findings in microbiome research, but also one where translation from animal studies to human applications has proven more complicated than early enthusiasm suggested.
The key study was conducted by Jeffrey Gordon's group at Washington University. In 2006, Turnbaugh et al.
published in Nature a demonstration that transplanting the microbiome from genetically obese mice into germ-free recipients caused those recipients to gain significantly more fat than recipients of microbiomes from lean donors - even though all mice ate the same diet.
The obese microbiome was more efficient at extracting energy from food, particularly through better fermentation of dietary polysaccharides to short-chain fatty acids.
The obese microbiome appeared to shift the balance between the two dominant bacterial phyla - Firmicutes (associated with more efficient energy extraction) and Bacteroidetes - toward Firmicutes.
In human studies, obese individuals did tend to have lower Bacteroidetes-to-Firmicutes ratios, and weight loss was associated with shifting this ratio. For a period, this became one of the most cited statistics in microbiome popular science.
However, subsequent larger and better-controlled human studies found the Firmicutes/Bacteroidetes ratio to be highly variable, inconsistent between populations, and not reliably predictive of obesity. The ratio varies enormously between healthy individuals depending on diet, geography, and other factors.
More recent work has shifted toward investigating specific bacterial species and their metabolic functions - particular organisms that produce or consume bile acids, affect appetite-regulating hormones like GLP-1 and PYY, or influence inflammation - rather than broad taxonomic ratios.
Akkermansia muciniphila, a mucus-layer-dwelling bacterium, has attracted particular attention as a potential beneficial organism associated with metabolic health and reduced intestinal permeability.
Fecal Microbiome Transplantation: A Genuine Success Story
Fecal microbiome transplantation (FMT) involves transferring processed stool from a healthy donor - containing a diverse microbial community - into the gastrointestinal tract of a recipient, typically via colonoscopy, enema, or oral capsules.
The goal is to restore a disrupted or dysbiotic microbiome by introducing a functioning community from a healthy donor.
The strongest evidence for FMT is in recurrent Clostridioides difficile infection (CDI). C. difficile is a toxin-producing bacterium that can overgrow the colon after antibiotic treatment has eliminated the normal protective microbiota. It causes severe diarrhea, colitis, and in serious cases life-threatening complications.
Recurrence rates after first-line antibiotic treatment are around 20-30% after a first episode and higher after subsequent ones.
A landmark 2013 randomized controlled trial published in the New England Journal of Medicine by van Nood et al. compared FMT by nasoduodenal infusion against standard antibiotic therapy for recurrent CDI.
FMT resolved infection in 81% of patients after a single infusion and 94% after a second infusion; standard vancomycin therapy resolved infection in only 31%.
The trial was stopped early because the FMT benefit was so clear that continuing the control arm was considered unethical.
Subsequent trials have confirmed cure rates in the 80-95% range, dramatically exceeding standard treatment. FMT for recurrent CDI is now recommended in clinical guidelines in most high-income countries.
Beyond CDI, FMT has been investigated for IBD, metabolic syndrome, autism spectrum disorder, and other conditions, but evidence remains limited and inconsistent.
Safety concerns - including the transmission of antibiotic-resistant organisms and at least two deaths from contaminated FMT products reported to the FDA - have underscored the need for rigorous donor screening and quality control.
FMT remains one of the clearest success stories in microbiome medicine while also illustrating how difficult it is to extrapolate from one well-defined indication to broader therapeutic use.
What the Evidence Shows About Probiotics
Probiotics are live microorganisms that, when administered in adequate amounts, confer a health benefit on the host - the definition from the WHO and FAO.
The commercial probiotic market is worth billions of dollars globally, and products are marketed for everything from digestive health to immunity to mental wellbeing. What does the rigorous evidence show?
Cochrane systematic reviews - meta-analyses of randomized controlled trials compiled by an independent international research network - provide the most reliable summaries. Cochrane reviews have found moderate-quality evidence supporting probiotics for:
- Preventing antibiotic-associated diarrhea in children and adults
- Preventing and treating acute infectious diarrhea
- Possibly reducing the incidence of necrotizing enterocolitis in preterm infants
For broader claims - general immune support, metabolic health, mental health, skin conditions in healthy adults - Cochrane and other systematic reviews consistently find insufficient evidence or null results.
The heterogeneity of probiotic products (different strains, doses, and formulations produce different effects), the lack of standardization, and industry funding bias in primary studies make it difficult to draw strong general conclusions.
Most healthy adults with intact microbiomes may experience little benefit from commercial probiotics, which often contain strains that do not persist in the gut after supplementation stops.
Personalized Nutrition and the Microbiome
A 2015 study from the Weizmann Institute by Eran Segal, Eran Elinav, and colleagues monitored continuous blood glucose responses in 800 people after standardized meals.
They found enormous inter-individual variation in glycemic response to identical foods - some people spiked glucose sharply after eating sushi while others did not, and vice versa for bread.
A machine learning algorithm incorporating microbiome composition (along with diet, activity, and other factors) could predict personalized glycemic responses more accurately than standard measures like glycemic index.
The study suggests that nutritional recommendations based on population averages may be less useful than individualized approaches informed by microbiome analysis.
However, this remains research-stage science; commercially available microbiome-based personalized nutrition services have not been validated against clinical outcomes in the way that would be required to make prescriptive recommendations.
"The microbiome is not a single entity but a community, and communities are not amenable to simple cause-and-effect stories. The science is real; the certainty with which it is being marketed is not."
- adapted from Eran Segal and Eran Elinav, The Personalized Diet (2017)
Key Terms in Microbiome Science
Microbiome: the totality of microorganisms and their genetic material in a defined environment (e.g., the gut microbiome).
Microbiota: the community of microorganisms themselves (without reference to their genomes).
Dysbiosis: an altered or disturbed microbial community, typically associated with reduced diversity or overgrowth of potentially harmful organisms.
Metagenomics: the study of genetic material recovered directly from environmental samples (including biological samples), bypassing the need for culture.
Short-chain fatty acids (SCFAs): metabolites produced by bacterial fermentation of dietary fiber in the colon. The principal SCFAs are butyrate, propionate, and acetate. Butyrate is the primary energy source for colonocytes (colon lining cells) and has anti-inflammatory effects.
Leaky gut: increased intestinal permeability, which allows bacterial products including lipopolysaccharide (LPS) to enter the bloodstream and trigger systemic inflammation. This is a real physiological phenomenon but has been significantly overhyped in popular health media.
16S rRNA sequencing: a standard method for identifying bacteria in a sample by sequencing a highly conserved but variable gene present in all bacteria. It identifies who is present but not what they are doing.
Shotgun metagenomics: sequencing all DNA in a sample, providing information about both the identity and functional capacity of the microbial community.
The microbiome field is at an important inflection point. The first generation of research - generating descriptive data about who is present in healthy versus diseased individuals - has largely been completed and found to be more complicated and less predictive than initially hoped.
The second generation - understanding mechanisms, establishing causation, and developing clinically useful interventions - is harder, slower, and less commercially spectacular, but it is where the durable science will be built.
For anyone navigating the substantial gap between current evidence and current commercial claims, the key question to ask of any microbiome-related product or recommendation is simple: what does a randomized controlled trial show, and was it conducted by investigators without financial interest in the outcome?
Frequently Asked Questions
How many microorganisms live in the human body, and why does the old 10:1 ratio get cited so often?
For decades, a widely repeated claim held that bacterial cells in the human body outnumber human cells by roughly ten to one, implying that we are ‘more microbe than human.’ The figure appeared in textbooks, popular science books, and countless articles. It originated from a back-of-envelope estimate made by microbiologist Thomas Luckey in 1972 that was never rigorously derived but became canonical through repetition.In 2016, Ron Sender, Shai Fuchs, and Ron Milo published a careful reassessment in Cell that revised the figure dramatically. Using updated estimates of both bacterial and human cell counts - and recognizing that the original calculation had overestimated bacterial density in the colon and underestimated the number of human cells - they concluded that the ratio is approximately 1.3:1, not 10:1. A 70-kilogram reference man contains roughly 38 trillion bacterial cells and approximately 30 trillion human cells. The margin of error in both estimates is large enough that the ratio could easily be near 1:1.This matters for more than precision. The 10:1 figure was used rhetorically to suggest that our microbial passengers constitute a kind of second organism, a hidden self. The corrected figure does not eliminate the microbiome’s importance - 38 trillion bacteria with collective genomes encoding metabolic functions our own genome lacks are still enormously significant - but it reframes the relationship. We are not ‘more microbe than human’; we are roughly co-equal in cell number, with microbes concentrated overwhelmingly in the colon.The episode is instructive about how quantitative claims circulate in science communication. A single poorly documented estimate became an accepted fact through repetition, citation from authority, and its narrative appeal. Sender et al.’s correction illustrates how numbers that seem precise can require surprisingly basic scrutiny.
What is the Human Microbiome Project and how did it change our understanding?
The Human Microbiome Project (HMP) was a major NIH initiative launched in 2007 and running through 2016 in two phases, with a budget exceeding $170 million. Its central goal was to characterize the normal microbial communities found at multiple body sites - gut, mouth, skin, vagina, nasal passages - in healthy adults, and to investigate how the microbiome relates to human health and disease.The project faced a fundamental technical challenge: the vast majority of human-associated microorganisms cannot be cultured in the laboratory under standard conditions, meaning traditional bacteriology could only see a fraction of the community. The HMP relied primarily on 16S ribosomal RNA gene sequencing, which targets a gene present in all bacteria but variable enough between species to serve as a molecular barcode. By sequencing the 16S gene from all DNA in a sample - a technique called amplicon sequencing - researchers could identify which organisms were present without needing to culture them. Shotgun metagenomics, sequencing all genetic material in a sample, added functional information: not just who is there but what metabolic capabilities they collectively encode.Key findings from the HMP and related projects included: (1) The human microbiome is enormously variable between individuals - more variable than the human genome. Two healthy people may share only about 30% of their gut bacterial species. (2) Body sites differ dramatically in their microbial communities. The vaginal microbiome is typically dominated by a single Lactobacillus species and is far less diverse than the gut; high diversity in the vaginal microbiome is associated with bacterial vaginosis rather than being beneficial as it is in the gut. (3) There is no single ‘healthy’ gut microbiome composition. Early claims about universal beneficial ratios of bacterial phyla have not held up. (4) The microbiome is functionally redundant: different communities can perform similar metabolic functions even with different species compositions.The HMP established the infrastructure and baseline data for the subsequent explosion of microbiome research, while also demonstrating that the field’s early enthusiasm for simple correlations would need to give way to more sophisticated analysis of function, causation, and individual variation.
How does the microbiome interact with the immune system?
The relationship between the gut microbiome and the immune system is one of the most important and best-documented aspects of microbiome science. It is also one where cause-and-effect relationships can be difficult to establish and where the science is still actively developing.The most compelling evidence comes from germ-free animal models. Mice raised in sterile conditions with no microbial colonization have profoundly abnormal immune systems: they have fewer and smaller lymph nodes and Peyer’s patches (immune tissue in the gut), lower levels of secretory IgA antibodies, and abnormal T-cell populations. Their immune systems are, in a technical sense, underdeveloped. Reintroducing specific bacteria partially or fully rescues these deficits, demonstrating that microbial signals during development are required for normal immune maturation.Particular bacterial communities have been identified as having specific immunological effects. Clostridia species in the colon - part of the normal human commensal community - induce the differentiation of regulatory T cells (Tregs), immune cells that suppress excessive inflammatory responses. Studies by Sarkis Mazmanian’s group and others showed that colonizing germ-free mice with a mixture of Clostridial strains restored normal Treg numbers and protected against experimental colitis and allergic responses. The practical implication is that disruption of these communities - for instance by broad-spectrum antibiotics in early life - might impair the calibration of immune tolerance.Epidemiological patterns support this. Inflammatory bowel diseases (Crohn’s disease and ulcerative colitis) are characterized by altered microbiome composition, though establishing whether dysbiosis causes IBD or results from it is methodologically challenging. The ‘hygiene hypothesis,’ reformulated as the ‘old friends hypothesis’ by Graham Rook, proposes that reduced exposure to the microorganisms with which humans co-evolved - particularly through industrialized sanitation, small family size, and antibiotic use - has left the immune system inadequately calibrated against inappropriate inflammatory responses, contributing to rising rates of allergies, asthma, and autoimmune conditions.
What is the gut-brain axis and how much does the microbiome actually affect mental health?
The gut-brain axis refers to the bidirectional communication network linking the central nervous system with the enteric nervous system (the extensive network of neurons embedded in the gut wall) and the gut microbiome. The communication runs through multiple channels: the vagus nerve, which carries signals between gut and brain stem; immune mediators including cytokines; the hypothalamic-pituitary-adrenal (HPA) axis regulating the stress response; and a range of metabolites produced by gut bacteria.One widely cited mechanism involves bacterial production of neurotransmitter precursors. Roughly 90-95% of the body’s serotonin is produced in the gut, not the brain, and several gut bacteria influence serotonin synthesis. Gut bacteria also produce gamma-aminobutyric acid (GABA), produce short-chain fatty acids that influence brain function, and can metabolize tryptophan through the kynurenine pathway relevant to mood regulation.Animal experiments have been striking. Transferring gut microbiota from anxious mouse strains into germ-free recipients produced anxiety-like behaviors; the reverse transfer also worked in some studies. Germ-free mice show altered stress responses and reduced anxiety relative to conventionally colonized mice, though this reverses if colonization occurs early in life. John Cryan and Ted Dinan coined the term ‘psychobiotics’ in 2013 to describe bacteria with potential mental health benefits.However, the field has significant problems with overclaiming. Human trials of probiotics for depression and anxiety have produced mixed results; most have been small, short-term, and methodologically limited. The most rigorous systematic reviews find modest effects at best. The mechanisms demonstrated in germ-free mouse models do not translate simply to humans with lifelong established microbiomes. The human gut-brain axis exists and is physiologically real, but confident claims that specific probiotic strains treat depression are currently ahead of the evidence. This is an active research area requiring caution in interpreting preliminary findings.
What does the science show about the microbiome and obesity?
The relationship between the gut microbiome and obesity is one of the most intriguing findings in microbiome research, but also one where the path from animal studies to human applications has proven more complicated than early enthusiasm suggested.The key study was conducted by Jeffrey Gordon’s group at Washington University. In 2006, Turnbaugh et al. published in Nature a demonstration that transplanting the microbiome from genetically obese mice into germ-free recipients caused those recipients to gain significantly more fat than recipients of microbiomes from lean donors - even though all mice ate the same diet. Follow-up work showed that the obese microbiome was more efficient at extracting energy from food, particularly through better fermentation of dietary polysaccharides to short-chain fatty acids that serve as caloric substrates. The obese microbiome appeared to shift the balance between the two dominant bacterial phyla - Firmicutes (associated with more efficient energy extraction) and Bacteroidetes - toward Firmicutes.In human studies, obese individuals did tend to have lower Bacteroidetes-to-Firmicutes ratios, and weight loss was associated with shifting this ratio. For a period, this became one of the most cited statistics in microbiome popular science. However, subsequent larger and better-controlled human studies have found the Firmicutes/Bacteroidetes ratio to be highly variable, inconsistent between populations, and not reliably predictive of obesity. The ratio varies enormously between healthy individuals depending on diet, geography, and other factors. The animal findings were real but the human translation was oversimplified.More recent work has shifted toward investigating specific bacterial species and their metabolic functions - particular organisms that produce or consume bile acids, that affect appetite-regulating hormones like GLP-1 and PYY, or that influence inflammation - rather than broad taxonomic ratios. Akkermansia muciniphila has attracted particular attention as a potential beneficial organism associated with metabolic health. Human intervention trials are underway but results remain preliminary.
What is fecal microbiome transplantation and what is the evidence for it?
Fecal microbiome transplantation (FMT) involves transferring processed stool from a healthy donor - containing a diverse microbial community - into the gastrointestinal tract of a recipient, typically via colonoscopy, enema, or oral capsules. The goal is to restore a disrupted or dysbiotic microbiome by introducing a functioning community from a healthy donor.The strongest evidence for FMT is in recurrent Clostridioides difficile infection (CDI). C. difficile is a toxin-producing bacterium that can overgrow the colon after antibiotic treatment has eliminated the normal protective microbiota. It causes severe diarrhea, colitis, and in serious cases life-threatening complications. First-line antibiotic treatment (metronidazole, vancomycin, or fidaxomicin) works initially but recurrence rates are high - around 20-30% after a first episode and higher after subsequent ones - because the antibiotics that treat C. difficile also suppress the normal microbiota that would otherwise prevent recurrence.A landmark 2013 randomized controlled trial published in the New England Journal of Medicine by van Nood et al. compared FMT by nasoduodenal infusion against standard antibiotic therapy for recurrent CDI. FMT resolved infection in 81% of patients after a single infusion and 94% after a second infusion; standard vancomycin therapy resolved infection in only 31%. The trial was stopped early because the FMT benefit was so clear that continuing the control arm was considered unethical. Subsequent trials have confirmed cure rates in the 80-95% range, dramatically exceeding standard treatment. FMT for recurrent CDI is now recommended in clinical guidelines.Beyond CDI, FMT has been investigated for IBD, metabolic syndrome, autism spectrum disorder, and other conditions, but evidence remains limited and inconsistent. Safety concerns - including the transmission of antibiotic-resistant organisms and at least two deaths from contaminated FMT products reported to the FDA - have underscored the need for rigorous donor screening and quality control. FMT remains one of the clearest success stories in microbiome medicine while also illustrating how difficult it is to extrapolate from one well-defined indication to broader therapeutic use.
What do Cochrane reviews actually say about probiotics, and what does personalized nutrition research suggest?
Probiotics are live microorganisms that, when administered in adequate amounts, confer a health benefit on the host - the definition from the WHO and FAO. The commercial probiotic market is worth billions of dollars globally, and products are marketed for everything from digestive health to immunity to mental wellbeing. What does the rigorous evidence show?Cochrane systematic reviews - meta-analyses of randomized controlled trials compiled by an independent international research network - provide the most reliable summaries. Cochrane reviews have found moderate-quality evidence supporting probiotics for preventing antibiotic-associated diarrhea in children and adults, preventing and treating acute infectious diarrhea, and possibly reducing the incidence of necrotizing enterocolitis in preterm infants. These are relatively specific indications with reasonable evidence bases.For broader claims - general immune support, metabolic health, mental health, skin conditions in healthy adults - Cochrane and other systematic reviews consistently find insufficient evidence or null results. The heterogeneity of probiotic products (different strains, doses, and formulations produce different effects), the lack of standardization, and industry funding bias in primary studies make it difficult to draw strong general conclusions. Most healthy adults with intact microbiomes may experience little benefit from commercial probiotics, which often contain strains that do not persist in the gut after supplementation stops.The personalized nutrition angle offers a more sophisticated picture. A 2015 study from the Weizmann Institute by Eran Segal, Eran Elinav, and colleagues monitored continuous blood glucose responses in 800 people after standardized meals. They found enormous inter-individual variation in glycemic response to identical foods - some people spiked glucose sharply after eating sushi while others did not, and vice versa for bread. A machine learning algorithm incorporating microbiome composition (along with diet, activity, and other factors) could predict personalized glycemic responses more accurately than standard measures like glycemic index. The study suggests that nutritional recommendations based on population averages may be less useful than individualized approaches informed by microbiome analysis. However, this remains research-stage science; commercially available microbiome-based personalized nutrition services have not been validated against clinical outcomes.