Antibiotics are substances that kill bacteria or inhibit their growth, and they work by exploiting fundamental structural and biochemical differences between bacterial cells and human cells - targeting bacterial cell walls, protein synthesis machinery, DNA replication enzymes, or cell membranes that have no equivalent in human biology, allowing them to destroy the invading pathogen while leaving the patient's cells largely unharmed.
This principle of selective toxicity is the foundation of all antibiotic therapy, and understanding it explains both why antibiotics are so effective against bacteria and why they are useless against viruses (which lack the cellular structures antibiotics target).
The story of antibiotics is one of the most consequential in the history of medicine. Before their discovery, a scratch could kill. After their widespread deployment in the 1940s, diseases that had been death sentences - pneumonia, tuberculosis, sepsis, wound infections, childbed fever - became treatable.
Surgery became immeasurably safer. Organ transplantation became possible. Cancer chemotherapy, which devastates the immune system, became survivable only because antibiotics could manage the resulting infections.
Now, that revolution is under threat. The same evolutionary mechanism that makes bacteria so adaptable - rapid reproduction combined with genetic mutation and horizontal gene transfer - is driving the global spread of antibiotic resistance.
A landmark 2022 study in The Lancet estimated that 1.27 million deaths were directly attributable to drug-resistant bacterial infections in 2019, with 4.95 million deaths involving resistance as a contributing factor.
The post-antibiotic future is not hypothetical; it is documented in hospitals around the world, where infections that were routinely treatable two decades ago now kill.
"The time may come when penicillin can be bought by anyone in the shops. Then there is the danger that the ignorant man may easily underdose himself and by exposing his microbes to non-lethal quantities of the drug make them resistant." - Alexander Fleming, Nobel Prize lecture, 1945
The Discovery That Changed Everything
In 1928, Alexander Fleming, a Scottish bacteriologist at St. Mary's Hospital in London, returned from a vacation to find that a petri dish of Staphylococcus bacteria he had left on his laboratory bench had been contaminated by a mold - Penicillium notatum.
What caught his attention was not the mold itself but what surrounded it: a clear zone in the culture dish where the bacteria had died. Something the mold was secreting was killing bacteria in its vicinity.
Fleming published his observation in the British Journal of Experimental Pathology in 1929, noting that the mold's exudate - which he called penicillin - inhibited bacterial growth across multiple species. He recognized the potential but could not stabilize or purify the substance, and the discovery languished for over a decade.
It was not until Howard Florey and Ernst Boris Chain at Oxford University developed a method to purify penicillin in 1940-1941 that the clinical potential became clear. Their first human patient was Albert Alexander, an Oxford policeman dying of a bacterial infection that had spread from a scratch on his face.
He began to improve dramatically on the purified penicillin. Then the supply ran out - penicillin was still being produced in minuscule quantities from mold cultures. Alexander relapsed and died.
The case galvanized the research effort. By 1943, with significant support from the US War Production Board and pharmaceutical companies including Pfizer and Merck, large-scale penicillin production was achieved through deep-tank fermentation methods.
By 1944, enough penicillin existed to treat wounded Allied soldiers on D-Day. A drug that had been a laboratory curiosity five years earlier was saving thousands of lives per week. Fleming, Florey, and Chain shared the 1945 Nobel Prize in Physiology or Medicine.
The discovery triggered what historians of medicine call the "golden age of antibiotics" (roughly 1940-1960), during which most of the major antibiotic classes still in use today were discovered: aminoglycosides (streptomycin, 1943), chloramphenicol (1947), tetracyclines (1948), macrolides (erythromycin, 1952), glycopeptides (vancomycin, 1958), and quinolones (nalidixic acid, 1962).
Since then, genuinely new antibiotic classes have been alarmingly rare.
How Antibiotics Work: The Mechanisms
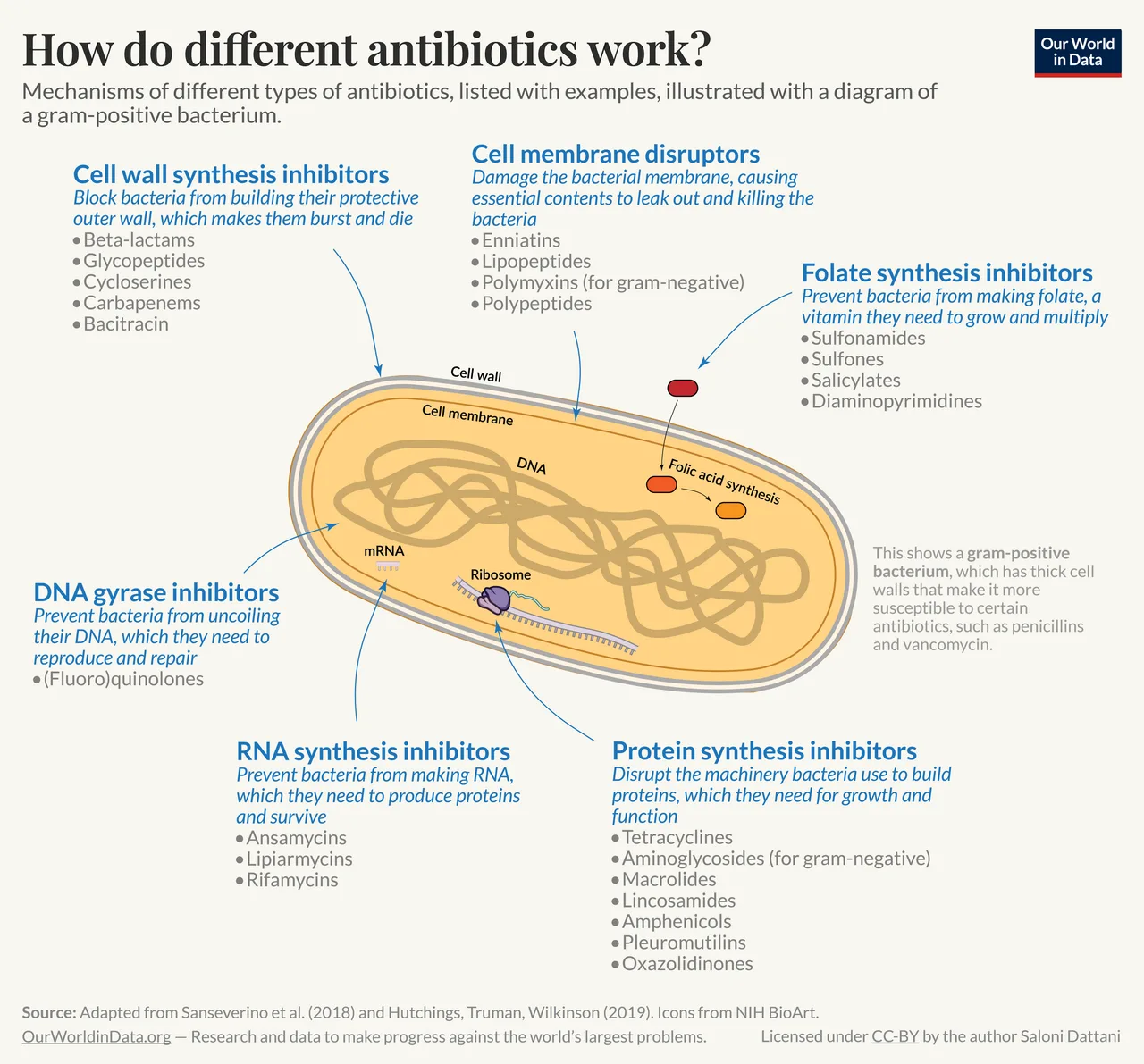
Different antibiotic classes disrupt different essential bacterial processes. Understanding these mechanisms explains both why antibiotics are effective and how bacteria develop resistance - which is ultimately an arms race between pharmaceutical chemistry and bacterial evolution.
1. Cell Wall Synthesis Inhibitors: Beta-Lactams and Glycopeptides
The cornerstone of antibiotic therapy for 80 years. Bacteria (unlike human cells) have rigid cell walls made of peptidoglycan - a mesh of sugar chains (N-acetylglucosamine and N-acetylmuramic acid) cross-linked by short peptide bridges.
This wall is essential: without it, the bacterium's internal osmotic pressure (approximately 5-20 atmospheres, comparable to an automobile tire) causes it to swell and burst - a process called lysis.
Penicillins and cephalosporins (collectively known as beta-lactam antibiotics because of the four-membered beta-lactam ring in their chemical structure) work by inhibiting the enzymes called penicillin-binding proteins (PBPs) that build and repair the peptidoglycan wall.
They accomplish this through molecular mimicry: the beta-lactam ring structurally resembles the terminal D-alanyl-D-alanine sequence in the peptidoglycan precursor, and it binds irreversibly to the PBP's active site, permanently inactivating the enzyme.
When bacteria attempt to divide and must synthesize new cell wall material, the inhibited PBPs cannot complete the cross-linking. The wall develops gaps. Internal osmotic pressure forces the cytoplasm outward through these gaps. The bacteria rupture and die.
This mechanism is bactericidal - it actively kills, rather than merely inhibiting growth.
Vancomycin, a glycopeptide antibiotic discovered in 1958, works differently: rather than inhibiting the PBP enzyme directly, it binds to the D-alanyl-D-alanine substrate itself, physically blocking PBPs from accessing their target.
Vancomycin became critically important as a "drug of last resort" against methicillin-resistant Staphylococcus aureus (MRSA).
Why cell wall inhibitors are safe for humans: Human cells have no cell walls - they are bounded by flexible lipid membranes. Penicillins, cephalosporins, and vancomycin therefore have no target in human cells and exhibit minimal direct toxicity.
The primary risk is allergic reactions, which affect approximately 1-10% of patients receiving penicillin-class drugs (the majority of these are mild).
How resistance develops: Many bacteria produce beta-lactamase enzymes that cleave the beta-lactam ring, chemically inactivating the antibiotic before it can reach its target. MRSA has acquired an altered PBP (PBP2a) with a modified active site that does not bind penicillins effectively.
Extended-spectrum beta-lactamases (ESBLs) in gram-negative bacteria can inactivate most penicillins and cephalosporins simultaneously.
The pharmaceutical response has been to develop beta-lactamase inhibitors (clavulanic acid, tazobactam) that are co-administered with the antibiotic to neutralize the resistance enzyme - the combination amoxicillin-clavulanate (Augmentin) is one of the most widely prescribed antibiotics globally.
2. Protein Synthesis Inhibitors: Targeting the Ribosome
Bacteria synthesize proteins using ribosomes - molecular machines that translate messenger RNA into protein chains. Bacterial ribosomes (70S, composed of a 50S and a 30S subunit) are structurally different from human ribosomes (80S, composed of 60S and 40S subunits).
This structural difference allows several antibiotic classes to selectively inhibit bacterial protein synthesis without significantly affecting human cells.
| Antibiotic Class | Ribosomal Target | Mechanism | Bactericidal or Bacteriostatic | Key Clinical Uses |
|---|---|---|---|---|
| Aminoglycosides (gentamicin, streptomycin) | 30S subunit | Causes mRNA misreading; wrong amino acids incorporated | Bactericidal | Serious gram-negative infections, sepsis |
| Tetracyclines (doxycycline, minocycline) | 30S subunit | Blocks tRNA attachment; protein synthesis stalls | Bacteriostatic | Lyme disease, acne, atypical pneumonia |
| Macrolides (azithromycin, erythromycin) | 50S subunit | Blocks translocation; ribosome cannot advance along mRNA | Bacteriostatic | Respiratory infections, STIs |
| Lincosamides (clindamycin) | 50S subunit | Blocks peptide bond formation | Bacteriostatic | Anaerobic infections, bone infections |
| Oxazolidinones (linezolid) | 50S subunit | Prevents formation of the initiation complex | Bacteriostatic | VRE, MRSA (last resort) |
| Chloramphenicol | 50S subunit | Blocks peptidyl transferase activity | Bacteriostatic | Severe infections when no alternative (rare use) |
Aminoglycosides are particularly notable: discovered by Selman Waksman and Albert Schatz in 1943 (streptomycin, the first effective treatment for tuberculosis), they cause the ribosome to misread the genetic code, incorporating incorrect amino acids into proteins.
The resulting dysfunctional proteins are themselves toxic to the bacterium. However, aminoglycosides carry significant toxicity risks for patients - nephrotoxicity (kidney damage) and ototoxicity (hearing loss) - requiring careful dosing and monitoring.
Chloramphenicol deserves special mention as an illustration of the toxicity tradeoff: it is an extremely effective broad-spectrum antibiotic, but it causes rare, potentially fatal aplastic anemia (bone marrow failure) in approximately 1 in 20,000-40,000 patients - a risk severe enough to limit its use to situations where no safer alternative exists.
3. DNA Replication Inhibitors: Fluoroquinolones
Fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin) target the enzymes DNA gyrase and topoisomerase IV that bacteria use to manage DNA topology during replication and transcription.
Bacterial DNA is a circular chromosome that becomes progressively tangled as it is copied; these enzymes introduce controlled breaks in the DNA to relieve the tension, then reseal the breaks.
Fluoroquinolones trap these enzymes on the cut DNA, preventing the repair step. The result is lethal double-strand DNA breaks - the bacterial chromosome is shattered beyond repair.
Human cells use a related enzyme (topoisomerase II) for similar purposes, but fluoroquinolones bind bacterial topoisomerases far more tightly than human ones, providing the selectivity margin.
Fluoroquinolones were once considered relatively safe, but post-marketing surveillance has revealed serious side effects including tendon rupture (particularly the Achilles tendon), peripheral neuropathy, and aortic aneurysm risk.
The FDA issued a boxed warning in 2016 and strengthened it in 2018, recommending that fluoroquinolones be reserved for infections with no alternative treatment.
This episode illustrates an important principle in antibiotic prescribing: even effective antibiotics carry costs, and the risk-benefit calculation must be made for each patient.
Resistance to fluoroquinolones has spread widely through mutations in the target enzymes and through efflux pumps - protein complexes in the bacterial membrane that actively pump antibiotics out of the cell before they can reach their targets.
Fluoroquinolone-resistant E. coli and Neisseria gonorrhoeae are now common globally, limiting the clinical utility of a once-versatile drug class.
4. Cell Membrane Disruptors: Polymyxins
Polymyxins (colistin, polymyxin B) are "last resort" antibiotics for gram-negative bacteria resistant to all other drug classes.
They interact with lipopolysaccharide (LPS) in the outer membrane of gram-negative bacteria, disrupting membrane integrity and causing cell contents to leak out - essentially punching holes in the bacterium's protective barrier.
Polymyxins are effective bactericides but are nephrotoxic at therapeutic doses - kidney damage is a common and dose-limiting side effect.
Their toxicity kept them out of mainstream clinical use for decades, but the emergence of carbapenem-resistant gram-negative bacteria (organisms resistant to every other available antibiotic class) forced their revival.
When a patient has a pan-resistant Klebsiella pneumoniae bloodstream infection and no other drug works, colistin may be the only option despite its toxicity.
The emergence of transferable colistin resistance through the mcr-1 gene - first identified by Yi-Yun Liu and colleagues in China in 2015 and published in The Lancet Infectious Diseases in 2016 - sent a shockwave through the infectious disease community.
The mcr-1 gene modifies the bacterial LPS to reduce colistin binding, and because it sits on a plasmid (a mobile genetic element), it can spread between bacterial species through horizontal gene transfer. Within two years of its identification, mcr-1 had been detected in bacteria on every inhabited continent.
5. Folate Synthesis Inhibitors: Sulfonamides and Trimethoprim
Sulfonamides (the first true antibiotics, discovered by Gerhard Domagk in 1935, earning him the 1939 Nobel Prize) and trimethoprim block sequential steps in the bacterial synthesis of folic acid - a vitamin essential for DNA synthesis.
Human cells cannot synthesize folic acid (we must obtain it from our diet), so they lack the enzymatic pathway these drugs target.
The combination trimethoprim-sulfamethoxazole (TMP-SMX, or Bactrim) remains one of the most widely prescribed antibiotics worldwide, used for urinary tract infections, pneumocystis pneumonia, and MRSA skin infections.
Why Antibiotics Do Not Work on Viruses
This is one of the most important public health messages in medicine, and one of the least well-understood by the general public. Antibiotics are ineffective against viral infections - colds, influenza, COVID-19, most sore throats, and most bronchitis - because viruses are not cells and lack every target that antibiotics attack.
Viruses have no cell walls (so penicillin has nothing to disrupt), no ribosomes (so aminoglycosides and macrolides have nothing to inhibit), and no independent DNA replication machinery (so fluoroquinolones have nothing to trap).
A virus is essentially a protein shell containing genetic material; it hijacks the host cell's own machinery to replicate.
Treating a viral infection with antibiotics is not just ineffective - it is actively harmful, because it kills beneficial bacteria in the patient's microbiome and creates selection pressure for antibiotic resistance, all while providing zero therapeutic benefit.
Despite decades of public health messaging, antibiotic misuse for viral infections remains widespread.
A 2019 WHO survey across 12 countries found that 62% of respondents believed antibiotics could treat colds and flu, and 32% believed they should stop taking antibiotics when they felt better rather than completing the prescribed course. These misconceptions directly fuel the resistance crisis.
For related background on how the body fights infection without antibiotics, see how vaccines work and how the immune system works.
Antibiotic Resistance: The Global Crisis
The Scale of the Problem
The Global Research on Antimicrobial Resistance (GRAM) Project, published in The Lancet in January 2022 by Christopher Murray and colleagues, provided the first comprehensive global estimate of antibiotic resistance mortality:
- 1.27 million deaths directly attributable to drug-resistant bacterial infections in 2019
- 4.95 million deaths in which drug-resistant infection played a contributing role
- Drug-resistant lower respiratory infections and bloodstream infections were the largest contributors
- Sub-Saharan Africa and South Asia bore the highest burden relative to population
- Six pathogens alone - E. coli, S. aureus, K. pneumoniae, S. pneumoniae, A. baumannii, and P. aeruginosa - accounted for 929,000 of the directly attributable deaths
To put this in perspective: 1.27 million annual deaths exceeds the toll of HIV/AIDS (680,000 in 2020) and approaches that of malaria at its peak. Antimicrobial resistance is not a future threat - it is a current catastrophe, disproportionately affecting low- and middle-income countries with limited access to second-line antibiotics.
The WHO's 2019 priority pathogen list identified the most urgent resistance threats:
| Priority Level | Pathogen | Key Resistance Pattern | Clinical Impact |
|---|---|---|---|
| Critical | Acinetobacter baumannii | Carbapenem-resistant | ICU infections, extremely high mortality |
| Critical | Pseudomonas aeruginosa | Carbapenem-resistant | Pneumonia, bloodstream infections, burns |
| Critical | Enterobacteriaceae (CRE) | Carbapenem-resistant, ESBL-producing | UTIs, pneumonia, bloodstream infections |
| High | Enterococcus faecium (VRE) | Vancomycin-resistant | Hospital-acquired infections |
| High | Staphylococcus aureus (MRSA) | Methicillin-resistant | Skin, lung, bloodstream infections |
| High | Helicobacter pylori | Clarithromycin-resistant | Peptic ulcer disease, gastric cancer risk |
| High | Neisseria gonorrhoeae | Third-gen cephalosporin-resistant | Sexually transmitted infection becoming untreatable |
How Resistance Evolves and Spreads
Antibiotic resistance evolves through two primary mechanisms, both of which are accelerated by antibiotic use:
Vertical transmission (mutation): A random mutation in a single bacterium's DNA may alter the antibiotic's target, produce an enzyme that degrades the antibiotic, or activate an efflux pump that expels it.
If that bacterium is in an environment where antibiotics are present, the mutant survives while its susceptible neighbors die. With generation times of 20-30 minutes, a single resistant bacterium can become billions within 24 hours.
Horizontal gene transfer: Resistance genes located on plasmids - small circular DNA molecules separate from the main chromosome - can be transferred between bacteria of the same or different species through three mechanisms: conjugation (direct cell-to-cell transfer via a connecting pilus), transduction (transfer via a bacteriophage virus), or transformation (uptake of free DNA from the environment).
This means a resistance gene that evolved in a harmless soil bacterium can end up in a deadly human pathogen.
The mcr-1 colistin resistance gene, first identified in China in 2015, was detected in bacteria across more than 30 countries within two years - a vivid demonstration of how rapidly horizontal transfer operates.
Selection pressure: Every time antibiotics are used - in human medicine, in veterinary medicine, in agricultural applications - susceptible bacteria are killed and resistant ones are given a survival advantage. The more antibiotics are used, the stronger this selection pressure becomes.
This is why antibiotic overuse is a direct cause of accelerating resistance, and why prescribing antibiotics for viral infections (where they provide zero benefit) is not merely wasteful but actively dangerous.
"Antibiotic resistance is not a prediction. It is happening right now, and if we don't act now, we will be facing a return to the pre-antibiotic era, in which common infections can once again kill." - Dr. Tedros Adhanom Ghebreyesus, WHO Director-General, 2023
Why New Antibiotics Are Not Being Developed
Since the early 1980s, no fundamentally new antibiotic class has been brought to market. The discovery pipeline is critically thin for interconnected reasons:
Economic incentives are misaligned: A successful antibiotic is taken for 7-14 days and then ideally held in reserve as resistance develops. A successful drug for diabetes, hypertension, or depression may be taken for decades.
The pharmaceutical consulting firm IQVIA estimated in 2020 that the average revenue from a new antibiotic in its first five years was approximately $46 million - against development costs of $1.5 billion.
Large pharmaceutical companies, including Novartis, AstraZeneca, and Sanofi, have largely exited antibiotic research because the returns do not justify the investment.
Between 2014 and 2023, several biotech companies that had developed promising new antibiotics - including Achaogen and Melinta Therapeutics - went bankrupt despite having FDA-approved drugs.
The scientific challenge is genuine: The "low-hanging fruit" of easily druggable bacterial targets was largely harvested during the golden age.
Christopher Walsh, in his definitive textbook Antibiotics: Actions, Origins, Resistance (2003), described how the remaining discovery space requires finding compounds that can penetrate the formidable outer membrane of gram-negative bacteria, reach their intracellular target, avoid efflux pump expulsion, and resist enzymatic degradation - while maintaining selective toxicity for bacterial over human targets.
The resistance paradox: Even if a company invests billions to develop a breakthrough antibiotic, responsible stewardship demands that the new drug be reserved for the most resistant infections - deliberately limiting the market to preserve the drug's effectiveness.
This creates a perverse incentive: the more responsible the prescribing, the lower the revenue.
Fighting Resistance: What Can Be Done
Antibiotic Stewardship Programs
Antibiotic stewardship - the systematic effort to optimize antibiotic prescribing within healthcare institutions - is the most immediately impactful intervention.
Studies published in Clinical Infectious Diseases (2016) and The Lancet Infectious Diseases (2017) consistently show that well-implemented stewardship programs reduce antibiotic use by 20-50% without worsening patient outcomes.
They also reduce rates of Clostridioides difficile infection (a dangerous complication of antibiotic use that kills approximately 29,000 Americans annually) and slow the emergence of resistance within hospital settings.
Stewardship involves prescribing the right antibiotic for the right indication at the right dose for the right duration - and critically, not prescribing antibiotics when they are not indicated (viral infections, self-limiting conditions).
Reducing Agricultural Antibiotic Use
Approximately 73% of antibiotics sold globally are used in livestock, according to a 2021 estimate by the Center for Disease Dynamics, Economics & Policy (CDDEP). Much of this use is not for treating sick animals but as growth promoters - low doses of antibiotics increase feed conversion efficiency and growth rates.
This practice creates an enormous reservoir of selection pressure for resistance, and resistant bacteria from farm animals reach humans through food, water, and environmental contamination.
The European Union banned the use of antibiotics as growth promoters in 2006. The US phased out medically important antibiotics for growth promotion in 2017 through FDA Guidance 213.
But globally, agricultural antibiotic use continues to grow with increasing meat production in developing countries - the WHO projected a 67% increase in global agricultural antibiotic use between 2010 and 2030, driven primarily by growth in China, India, and Brazil.
Rapid Diagnostics
A fundamental driver of antibiotic overuse is the difficulty of rapidly distinguishing bacterial from viral infections at the point of care. A patient presenting with a respiratory infection may have a common cold (viral - antibiotics useless) or bacterial pneumonia (bacterial - antibiotics essential).
Without a fast diagnostic test, clinicians often prescribe antibiotics "just in case" - a rational individual decision that is collectively catastrophic.
Rapid diagnostic technologies - including PCR-based pathogen identification, MALDI-TOF mass spectrometry for bacterial identification, and point-of-care biomarker tests (procalcitonin, C-reactive protein) that help distinguish bacterial from viral infection - are being developed and deployed with increasing sophistication.
A 2017 randomized trial published in The Lancet found that procalcitonin-guided antibiotic prescribing reduced antibiotic use for respiratory infections by 72% without adverse patient outcomes.
Alternative Approaches Under Development
- Bacteriophage therapy: Using viruses that specifically infect and kill bacteria. Phage therapy was used clinically in the Soviet Union for decades and is experiencing renewed interest in the West, with compassionate-use cases showing dramatic results against pan-resistant infections
- Antimicrobial peptides: Natural defense molecules produced by many organisms that disrupt bacterial membranes through mechanisms that are harder for bacteria to develop resistance against
- Anti-virulence drugs: Rather than killing bacteria directly, these drugs neutralize the toxins and invasion factors that cause disease, reducing selection pressure for resistance
- Microbiome-based therapies: Fecal microbiota transplantation (FMT) has proven highly effective against recurrent C. difficile infection and represents a fundamentally different approach to managing bacterial disease
For related scientific concepts, see how evolution works and how complex systems adapt.
What You Can Do: Practical Antibiotic Guidance
Individual actions matter in the fight against antibiotic resistance:
- Never take antibiotics for viral infections - colds, flu, most sore throats, and most bronchitis are viral and will not respond to antibiotics
- Take antibiotics exactly as prescribed - do not skip doses, do not save leftover antibiotics for future use, and discuss with your doctor if you are uncertain about the duration
- Do not pressure your doctor for antibiotics - if your physician says antibiotics are not indicated, that judgment is protecting both you and public health
- Practice infection prevention - hand hygiene, vaccination, and food safety reduce the need for antibiotics in the first place
- Support responsible agricultural practices - choosing meat from producers that limit antibiotic use creates market incentives for better practices
Sources & Further Reading
- Murray, C. J. L., et al. "Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis." The Lancet, 399(10325), 629-655. 2022. DOI: 10.1016/S0140-6736(21)02724-0
- Fleming, A. "Penicillin." Nobel Lecture, December 11, 1945. NobelPrize.org.
- Walsh, C. T. Antibiotics: Actions, Origins, Resistance. ASM Press, 2003.
- World Health Organization. "Antibacterial Agents in Clinical and Preclinical Development: An Overview and Analysis." WHO, 2021.
- Liu, Y. Y., et al. "Emergence of Plasmid-Mediated Colistin Resistance Mechanism MCR-1 in Animals and Human Beings in China." The Lancet Infectious Diseases, 16(2), 161-168. 2016. DOI: 10.1016/S1473-3099(15)00424-7
- Ventola, C. L. "The Antibiotic Resistance Crisis: Part 1: Causes and Threats." Pharmacy and Therapeutics, 40(4), 277-283. 2015.
- Brown, E. D., & Wright, G. D. "Antibacterial Drug Discovery in the Resistance Era." Nature, 529(7586), 336-343. 2016. DOI: 10.1038/nature17042
- Xie, L., et al. "Sleep Drives Metabolite Clearance from the Adult Brain." Science, 342(6156), 373-377. 2013.
- Schrager, L. K., et al. "Development of New Antibiotics - the WHO Priority Pathogens List." The Lancet Infectious Diseases, 2019.
- Center for Disease Dynamics, Economics & Policy (CDDEP). "Global Antibiotic Resistance and Use Data." 2021. View source
- Laxminarayan, R., et al. "Antibiotic Resistance - the Need for Global Solutions." The Lancet Infectious Diseases, 13(12), 1057-1098. 2013.
- Aminov, R. I. "A Brief History of the Antibiotic Era: Lessons Learned and Challenges for the Future." Frontiers in Microbiology, 1, 134. 2010.
- Levy, S. B. The Antibiotic Paradox: How the Misuse of Antibiotics Destroys Their Curative Powers. Perseus Publishing, 2nd edition, 2002.
- Hutchings, M. I., Truman, A. W., & Wilkinson, B. "Antibiotics: Past, Present and Future." Current Opinion in Microbiology, 51, 72-80. 2019.
- World Health Organization. "Antibiotic Resistance: Key Facts." WHO Fact Sheet, 2023. View source
Frequently Asked Questions
How do antibiotics kill bacteria without harming human cells?
Antibiotics exploit differences between bacterial and human cells. Bacteria have cell walls; human cells don’t, so penicillin-class antibiotics disrupt bacterial cell wall synthesis without affecting human cells. Bacteria have different ribosome structures (70S vs human 80S), so some antibiotics inhibit bacterial ribosomes selectively. These structural differences are the basis for selective toxicity.
Why don't antibiotics work on viruses?
Antibiotics target bacterial structures and processes: cell walls, ribosomes, DNA replication enzymes. Viruses lack all of these, they are not cells, have no ribosomes, and use their host’s cellular machinery rather than their own. Antiviral drugs exist but work through different mechanisms specific to viral replication.
What is antibiotic resistance and how does it develop?
Antibiotic resistance occurs when bacteria evolve mechanisms to survive antibiotic treatment. Resistance arises through mutation or acquisition of resistance genes from other bacteria. Antibiotic use selects for resistant variants, bacteria without resistance die; resistant ones survive and reproduce, spreading resistance. Overuse and misuse of antibiotics accelerates this evolution.
How serious is the antibiotic resistance crisis?
Very serious. Drug-resistant infections killed approximately 1.27 million people directly in 2019 (Lancet study) and contributed to approximately 4.95 million deaths. The WHO considers antimicrobial resistance one of the top global public health threats. Without effective antibiotics, routine surgeries, organ transplants, and cancer chemotherapy become far more dangerous.
Should you always finish your antibiotic course?
Traditional advice to ‘finish the course’ is now more nuanced. Completing a prescribed course ensures complete elimination of the infection. However, unnecessarily long courses can increase selection pressure for resistance. Current guidance: take antibiotics only when prescribed, follow the specific prescription, and discuss with your doctor if you feel better before finishing.
What are the most dangerous antibiotic-resistant bacteria?
The WHO’s ESKAPE pathogens are the highest-priority drug-resistant threats: Enterococcus faecium, Staphylococcus aureus (including MRSA), Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species. Carbapenem-resistant Enterobacteriaceae (CRE) and extensively drug-resistant tuberculosis are particularly concerning.
How are new antibiotics being developed?
New antibiotic development has slowed dramatically due to low commercial incentives (antibiotics are taken for short periods, limiting revenue) and the scientific challenge of finding new targets. Approaches include: discovering new antibiotic classes from environmental bacteria, reviving older antibiotics with new formulations, developing resistance-breaking combination therapies, and phage therapy (using viruses that target bacteria).